In the previous posts we applied LDA topic modeling to text documents from data collected from the subreddit depressionregimens. Here I will continue with the results from the derived topics model – obtaining the most representative text for each topic. As was stated, the chosen model has ten topics, and LDA assumes that each document is composed of multiple topics, with each topic being assigned a probability. Each topic is composed of multiple words, with each word assigned a probability.
Previous post: Reddit Depression Regiments – Topic Modeling
Since each document is composed of multiple topics, for each topic we can find a document with the highest probability for that topic, therefore that will be our most representative document.
Topic 1
(‘feel’, 0.040), (‘year’, 0.026), (‘thing’, 0.022), (‘symptom’, 0.020), (‘brain’, 0.019), (‘start’, 0.018), (‘time’, 0.017), (‘make’, 0.015), (‘issue’, 0.015), (‘lot’, 0.014)
Most representative post id with topic 1 probability of 0.45:
Full text here: https://www.reddit.com/r/depressionregimens/comments/gib17h
“Blank Mind Syndrome” – Sub group of specific symptoms including: – Loss of Internal Monologue, lack of coherent automatic thoughts, no track of time passage, lack of self insight – Depersonalisation/Derealization Feeling detached, having no “sense of self”, missing mental features, having no emotional autobiography, feeling as if every day is the same, loss of relationship or emotional attachments, feeling detached from external reality – Cognitive Decline, Loss of Visual imagination, inability to think in a deep or complex way, inability to hold information, loss of past learned skills and knowledge. – Complete Lack of goal-directed motivation, having no automatic self direction, no long term goals – Anhedonia – inability to enjoy or derive pleasure, nothing to look forward to, no bodily joy, satasfaction and so on – Lack of atmosphere/deepness of the outside reality, inability to appreciate beauty, things look flat and insignificant. All symptoms in various severity of course, It’s time to talk, what is this condition exactly, Did you suffer from depression your entire life? Is this episodic? how are you planning to solve it? how did you acquire it? had any professional been aware of it? Is it medication induced? Is there any outside outlet acknowledging this specific phenomena? How much time do you suffer from it? What were you diagnosed with? Was it sudden or progressively? Had anything helped at all? Would you join a group for people suffering the same condition? Is anyone interested in doing so? Please do respond!
Topic 2
people 0.044, depression 0.037, doctor 0.028, psychiatrist 0.020, make 0.020, bad 0.016, therapy 0.016, therapist 0.015, find 0.014, problem 0.013
Most representative post for this topic, with probability for topic 2 of 0.53: https://www.reddit.com/r/depressionregimens/comments/iij4tr
I talked to him today, he says all my problems are my choice and I choose to be lazy, suicidal, depressed etc. Is he right?,Dude… if he believes this then he must also believe that his career is total quackery. Get a new psychiatrist immediately. What a piece of shit.,absolutely not, please get a new psychiatrist!! you don’t choose to be suicidal or depressed, and in my experience, depression causes laziness more often than not. it’s worrisome that a professional outright said this to you and honestly I would report him if you can. that’s such a harmful thing to say to anyone suffering from such issues and to say it to the wrong person could be really catastrophic. i’m sorry he’s a dick to you, don’t listen to his bullshit. if it was so easy as to choose not to be depressed then nobody would fucking be depressed. it’s like he thinks people enjoy feeling this way ugh,OMG please please PLEASE never go back there. I once had a psychiatrist tell me I was gonna end up on a street corner with a sign (spoiler alert: I have a career and own a house). I got up and left and never looked back. Remember that YOU are a huge part of your mental health journey. It’s a collaborative effort between you, your psychiatrist, therapist (if you have one), and any other professional you choose to involve. You always have a say, and if something doesn’t seem right, you don’t have to go along with it. Your feelings are ALWAYS valid—don’t ever let anyone tell you differently. You are not alone in this. So many of us are depressed, anxious, suicidal, attention deficit, bipolar, lazy…these are NOT choices. Who would choose to be this way? There are plenty of helpful professionals out there, just make sure you screen them carefully. I believe in you and wish you well!!! …
Topic 3
day 0.037, thing 0.035, feel 0.033, make 0.024, find 0.017, good 0.016, exercise 0.016, eat 0.013, walk 0.013, lot 0.013
https://www.reddit.com/r/depressionregimens/comments/dztdw9
Topic probability: 0.53
Wanted to share something that I’ve recently found to help when I’m struggling to find motivation to complete basic chores. This one specifically deals with laundry, but it can apply to other tasks as well. If you’re like me, you can have laundry sitting there for weeks not being put away. The mountain of clothing is so overwhelming that I just ignore it all together. I’m also an all-or-nothing person; I just wait and wait until a good day when I’ll have enough energy to get it done. Those days are exceedingly rare, so that mountain of clothes will sit there for a loooong time, stressing me out and depressing me even more. I’m trying to switch my mindset to not feeling like I need to take on such giant tasks all at once. I decided to break up the tasks into smaller ones. For the mixed load of laundry that needed to be put away, I told myself I only need to put away the socks and underwear today. Then tomorrow I put away the shirts. The next day, fold pants, and the next everything else that goes on hangers. These smaller tasks only take like 5-10 minutes each, and it’s satisfying to see the pile of clothes dwindle every day versus sit there ominously for several weeks. If you’re feeling overwhelmed, break up your tasks into very small, easily attainable goals. Go easy on yourself and do what you can for the day. Even just the tiniest amount of progress is a good thing.,great advice. Anytime you get anxiety over a task or a situation seems to complex or overwhelming. Just break in down into manageable pieces. Doing SOMETHING is always better than nothing even if it seems like too little or not enough or w/e.,I saw a meme about ‘anything worth doing is worth doing badly’ that addresses this. I try and remember that some days. Us perfectionists want to always do 100%. But in a lot of things (not everything, obviously, just as a general rule) doing 50% of the job, or 90% of the job, is way better then the 0% of the job we do because of that crippling dedication to doing 100%. Not an excuse for doing bad jobs on the stuff that really matters, but can be a much healthier way to approach doing general day-to-day stuff…
Topic 4
ssris 0.027, antidepressant 0.024, effect 0.024, drug 0.022, side_effect 0.020, depression 0.019, serotonin 0.016, prescribe 0.014, treat 0.013, ssri 0.012
Reddit post: https://www.reddit.com/r/depressionregimens/comments/bheg7d
Topic probability: 0.64
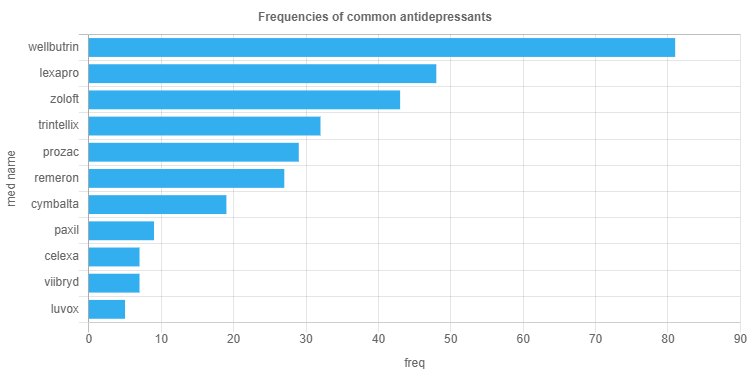
Hey y’all, this is a repost of the stickied post made by /u/jugglerofworlds, who appears to have deleted their account and their post along with it. I’ve edited it a little and will continue to keep it updated as needed. Suggestions are welcome. As the former post was, I’m trying to keep this confined to prescription medications, and not natural/herbal remedies (though I recognize that they definitely can be helpful means of treatment). I’m also typically avoiding medications that have been withdrawn from the market and thus aren’t really prescribed. In a future revision of this post I hope to add an additional column featuring which medications are available where, as some of these are approved in European countries but not in the U.S., and vice versa. # Icon key * ✔️ = approved to treat condition by a regulatory agency (FDA, EMA, ANSM, etc) * ➕ = approved as an adjunct treatment by a regulatory agency, to be used in combination with other medications to treat a condition (may or may not be used off-label as a monotherapy) * 🏷️ = Off label use; widely prescribed for condition but not necessarily rigorously studied for it * ⚠️ = experimental medication; in FDA Phase III trials or pending approval # Selective Serotonin Reuptake Inhibitors (SSRIs) |Generic name|Brand name(s)|Treats depression|Treats anxiety| |:-|:-|:-|:-| |citalopram|Celexa|✔️|🏷️| |escitalopram|Lexapro|✔️|✔️| |fluoxetine|Prozac|✔️|✔️| |fluvoxamine|Luvox/Luvox CR|✔️|✔️| |paroxetine|Paxil/Paxil CR|✔️|✔️| |sertraline|Zoloft|✔️|✔️| # Serotonin Modulator and Stimulators (SMS) |Generic name|Brand name(s)|Treats depression|Treats anxiety| |:-|:-|:-|:-| |vortioxetine|Trintellix|✔️|🏷️| |vilazodone|Viibryd|✔️|🏷️| # Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) |Generic name|Brand name(s)|Treats depression|Treats anxiety| |:-|:-|:-|:-| |venlafaxine|Effexor/Effexor XR|✔️|✔️| |desvenlafaxine|Pristiq|✔️|🏷️| |duloxetine|Cymbalta|✔️|✔️| |milnacipran|Savella|✔️|✔️| |levomilnacipran|Fetzima|✔️|🏷️| |atomoxetine|Strattera|⚠️|⚠️| # Tricyclics (TCAs) ## TCAs with a preference for serotonin |Generic name|Brand name(s)|Treats depression|Treats anxiety|…
Topic 5
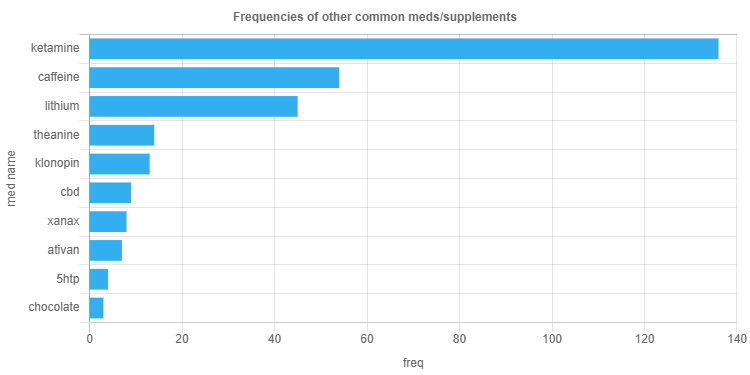
treatment 0.035, ketamine 0.028, year 0.022, work 0.021, drug 0.017, hope 0.015, hear 0.012, lithium 0.011, people 0.010, infusion 0.009
Reddit post: https://www.reddit.com/r/depressionregimens/comments/axtnj8
Topic probability: 0.58
https://www.washingtonpost.com/health/2019/03/06/biggest-advance-depression-years-fda-approves-novel-treatment-hardest-cases The Food and Drug Administration approved a novel antidepressant late Tuesday for people with depression that does not respond to other treatments — the first in decades to work in a completely new way in the brain. The drug, a nasal spray called esketamine, has been eagerly anticipated by psychiatrists and patient groups as a powerful new tool to fight intractable depression. The spray acts within hours, rather than weeks or months as is typical for current antidepressants, and could offer a lifeline to about 5 million people in the United States with major depressive disorder who haven’t been helped by current treatments. That accounts for about one in three people with depression. “This is undeniably a major advance,” said Jeffrey Lieberman, a Columbia University psychiatrist. But he cautioned much is still unknown about the drug, particularly regarding its long-term use. “Doctors will have to be very judicious and feel their way along,” he said. The label for the drug will carry a black box warning – the most serious safety warning issued by the FDA. It will caution users they could experience sedation and problems with attention, judgment and thinking, and that there’s potential for abuse and suicidal thoughts. People who take esketamine will have to be monitored for at least two hours after receiving a dose to guard against some of these side effects…
Topic 6
work 0.053, anxiety 0.030, mg 0.025, bad 0.020, high 0.020, vitamin 0.018, diet 0.015, supplement 0.014, post 0.012, literally 0.011
Reddit post: https://www.reddit.com/r/depressionregimens/comments/alh4r3
Topic probability: 0.52
About 3 or 4 years ago, I developed a severe form of anxiety disorder where it manifested in panic attacks characterized by intense bouts of nausea, gagging, and retching. It didn’t usually get bad enough to get to vomiting, though it did in a few instances (in which I went to the hospital afterwards). My body responds to stress naturally by gagging and nausea. So imagine being anxious all the time but also NAUSEOUS 24/7, and I mean literally 24/7 without any respite. At times I was seriously considering suicide because of how bad I felt all the time every day. The whole thing started I think because I had to present at a large conference with thousands of people in attendance, and I had a very bad experience being insulted by some people at a previous iteration of this conference years ago. I was commuting to work one day (before the conference) and suddenly got this massive bout of nausea where I felt like I was dying. I realized however that this was my body telling me I have stagefright. I expected my nausea to evaporate once I finished speaking, as it usually would have in the past. Except that it didn’t. It stayed, and remained with me for years. I tried everything but avoided antidepressants for the longest time due to the bad rep they get. I tried the following medications: * Ginger – in various forms – for nausea (didn’t work) * Peppermint – in various forms – for nausea (didn’t work) * Ondansetron (zofran) – 4 mg; as needed – for nausea (didn’t work) * Chlordiazepoxide/clidinium bromide (librax) – 5 mg; once daily – for nausea and anxiety (didn’t work) * Pyridoxine/doxylamine (diclectin) – 10 mg pyridoxine, 10 mg doxylamine; 2 tablets at bedtime – for nausea (didn’t work) * Metoclopramide – 1 tablet daily – for nausea (didn’t work) * Domperidone – 10 mg; once daily – for nausea (didn’t work) * Propranolol – 10 mg; twice daily – for anxiety (didn’t work) * Prochlorazapine – 10 mg; twice daily – for nausea (didn’t work) * Lorazepam (Ativan) – 1 mg; 1 tablet at bedtime – for anxiety (didn’t work; just made me really sleepy) * Pantoprazole (Tecta) – 1 tablet daily – for nausea (didn’t work) * Dimenhydrinate (Gravol) – 1 tablet as needed – for nausea (didn’t work) * Nabilone (cesamet) – 0.5 mg as needed – for nausea (worked for nausea but not anxiety, and gave me a really uncomfortable high) * Clomipramine (Anafranil) – 10 mg. once daily – for anxiety (didn’t try properly due to side-effects) I was afraid even of getting out of my own house. I was afraid of meeting people. I was afraid of leaving my own room – the only place where I felt somewhat at ease and the nausea wasn’t THAT bad. The only thing that worked somewhat to relieve the nausea was chewing on things, whether that meant food at mealtimes, or fennel seeds, or sucking on mints/cough drops. So I carried mints and fennel seeds with me at all times no matter where I was – including in the washroom in my own house and even when I wanted to take a shower I had to have them nearby otherwise I would literally throw up in the shower. But these were not long-term cures to my problem and only a short alleviation of the symptoms (and not that effective if I was more anxious than usual). I somehow graduated from university with a degree in neuroscience and fought through this nausea-anxiety for 2 years doing so. My graduation ceremony – which was supposed to be a happy occasion – was marred by constant nausea and me going through at least 3 entire tins of mints because my body handles excitedness the same way as it does for anxiety. Literally nothing was working and I was at my wit’s end. So I went downtown Toronto and bought CBD oil from a dispensary. I only did this because I was literally desperate, even though I had never done any recreational drugs in my life upto that point (except caffeine), and even though I had a horrible experience with nabilone (synthetic THC for cancer patients to reduce their nausea) so I was really kind of anxious about even using that. But it worked…