Here I will list different medications, supplements, and procedures that are used to treat depression, anxiety, and obsessive/suicidal thoughts. I am not suggesting that you go out and buy a bunch of antidepressants and try them one by one, I just want you to be aware of what exists out there so that you can discuss this with your doctor. Some things, such as a daylight lamp, or omega 3s, don’t require prescription. Since I have been dealing with autoimmune encephalitis for more than three years already, I have tried most of these treatments in attempts to reduce my depressive symptoms, psychosis, and intrusive thoughts.
Many people do get better with antidepressants. I have to note though, that in my case, the most useful treatment was high-dose intravenous steroids (IV Solu-Medrol) for five days. I did have severe psychotic depression with suicidal tendencies, my neurologist and psychiatrist propose that this was due to autoimmune encephalitis (Hashimoto’s encephalitis) – brain inflammation. Many people have milder depression and do well after antidepressant treatment. My state has improved but it is not without moments of intrusive thoughts and for this reason I continue trying different methods.
Medication
Antidepressants


How does your psychiatrist determine which antidepressant to try? It seems that in general this is not based on any specific medical tests, but is based on the discussion with you about your symptoms. I did get a genetic test done on my saliva. This was part of CAMH Impact Study in Toronto, the provided report is called GeneSight Psychotropic Test. The company states that their test “analyzes how your genes affect your response to psychotropic medications commonly prescribed to treat depression, anxiety, bipolar disorder, posttraumatic stress disorder (PTSD), obsessive compulsive disorder, schizophrenia and other behavioral health conditions. There are dozens of medications used to treat depression and other mental illnesses and selecting the right antidepressant medication or other medication can be a challenging and frustrating process. GeneSight Psychotropic’s genetic testing enables your clinician to identify and avoid depression, anxiety and/or other medications that are unlikely to work or may cause side effects.” This test was provided to me for free by CAMH in Toronto.
GeneSight Psychotropic Test link
New antidepressants:
There are three new antidepressants that have become recently available in US and Canada – vortioxetine, levomilnacipran extended-release (ER), and vilazodone. Vortioxetine – may enhance serotogenic activity via reuptake inhibition of serotonin receptors. Levomilnacipran is a a serotonin norepinephrine reuptake inhibitor. Vilazodone is a serotonin reuptake inhibitor and partial serotonergic 5-HT1A receptor agonist.
The role of new antidepressants in clinical practice in Canada: a brief review of vortioxetine, levomilnacipran ER, and vilazodone
Antipsychotics
Sometimes antipsychotics are added to antidepressants during treatment. Usually antipsychotics are used to treat schizophrenia, why are they given to depressed patients? I think the reason is that many patients don’t achieve remission with antidepressants, so other medications/methods must be tried. In the large National Institute of Mental Health Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial, only about 30% of patients achieved remission (virtual absence of depressive symptoms) after up to 12 weeks of first-line treatment with citalopram. Evidence of the usefulness of atypical antipsychotics in treating MDD goes back more than 7 years (statement from 2009). A controlled trial found that the combination of olanzapine and fluoxetine was more helpful in treating patients with MDD (without psychosis) than fluoxetine or olanzapine alone.2 The group that received combination therapy did significantly better than the others. In November 2007, the FDA approved aripiprazole as the first atypical antipsychotic to treat MDD. It is specifically for adjunctive treatment, along with an antidepressant, for the treatment of refractory MDD.
Atypical Antipsychotics for Treating Major Depression
Aripiprazole (Abilify) – was approved by FDA for major depressive disorder in 2007, for patients who had inadequate response to antidepressants. Aripiprazole is a partial agonist at dopamine D(2) and D(3) and serotonin 5-HT1A receptors, and is an antagonist at 5-HT(2A) receptors.
Ripseridone – risperidone has actions at several 5-HT (serotonin) receptor subtypes. A study showed that depression symptoms improved modestly but significantly more in the risperidone group compared with the placebo group, as measured by clinician-rated symptom response and patient-rated self-assessment. The 17-item Hamilton Rating Scale for Depression score improved more in the risperidone group versus the placebo group.
Quetiapine (Seroquel) – quetiapine is a dopamine, serotonin, and adrenergic antagonist, and a potent antihistamine with some anticholinergic properties. Quetiapine binds strongly to serotonin receptors; the drug acts as partial agonist at 5-HT1A receptors. One study involved more than 700 people who had suffered from depression for at least one month but less than one year. Patients were randomly assigned to take one of three doses of Seroquel or a placebo once a day for six weeks. Those taking Seroquel showed greater improvement in depression symptoms than those on placebo.
Supplements
St. John’s Wort – hypericum perforatum, it is a flowering plant. Sold in health stores/drug stores/online. A 2008 review of 29 international studies suggested that St. John’s wort may be better than a placebo and as effective as different standard prescription antidepressants for major depression of mild to moderate severity. A 2015 meta-analysis review concluded that it has superior efficacy to placebo in treating depression, is as effective as standard antidepressant pharmaceuticals for treating depression, and has fewer adverse effects than other antidepressants.[23] The authors concluded that it is difficult to assign a place for St. John’s wort in the treatment of depression owing to limitations in the available evidence base, including large variations in efficacy seen in trials performed in German-speaking relative to other countries. In Germany, St. John’s wort may be prescribed for mild to moderate depression, especially in children and adolescents.
Omega – 3 – omega-3 fatty acids are found in oily fish such as salmon. You can also purchase fish oil supplements in health stores/online. In general eating oily fish is considered to be a healthy choice. There is some evidence that omega-3s might help with depression, but this evidence is not very strong. From Cochrane review: “At present, we do not have enough high quality evidence to determine the effects of n-3PUFAs as a treatment for MDD. We found a small-to-modest positive effect of n-3PUFAs compared to placebo, but the size of this effect is unlikely to be meaningful to people with depression, and we considered the evidence to be of low or very low quality, with many differences between studies.“
SAMe – S-adenosyl-L-methionine (SAMe) is a compound found naturally in the body. SAMe helps produce and regulate hormones and maintain cell membranes. A synthetic version of SAMe is available as a dietary supplement in the U.S. In Europe, SAMe is a prescription drug. From Cochrane review: “We included eight studies involving 934 people in this review. There was no strong evidence of a difference in effectiveness between SAMe and imipramine or escitalopram when used alone. It was superior to placebo when used in combination with selective serotonin reuptake inhibitor antidepressants, but this evidence was of low quality. There was no significant difference in terms of effectiveness between SAMe and placebo alone, but again this evidence was of very low quality.“
Folic acid – also known as vitamin B9. Foods that are naturally high in folate include leafy vegetables (such as spinach, broccoli, and lettuce), okra, asparagus, fruits (such as bananas, melons, and lemons) beans, yeast, mushrooms, meat (such as beef liver and kidney), orange juice, and tomato juice.
“The evidence for a link between depression and folate levels comes from various sources. Along with vitamins B6 and B12, folate helps break down the amino acid homocysteine. High blood levels of homocysteine are associated with Alzheimer’s disease and depression, although a cause-and-effect relationship hasn’t been proven. The breakdown of homocysteine generates SAMe, a major constituent of brain cells and, some think, a possible treatment for depression. Low levels of SAMe might explain any connection between folate and depression.”
Folate for depression
Probiotics – there is one combination of two bacterial strains that has shown some promise in treating mental health issues. Bifdobacterium longum R0175 and L. helveticus R0052 have been found to reduce symptoms of stress and anxiety. In Canada there are two brands with these strains – CalmBiotic and Jamieson Probiotic Sticks.
Clinical Guide to Probiotic Products Available in Canada
Other things to consider
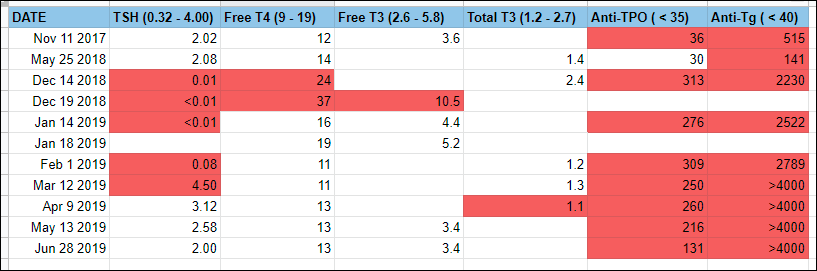
- Getting tested for hypo/hyperthyroidism – potential need for thyroid hormones
Treating an underactive thyroid gland may improve mood
- Getting tested for anemia
Sometimes the first symptoms of iron deficiency are neurologic
- Getting tested for coeliac disease – possible benefit from excluding gluten from diet
The Link between Celiac Disease and Depression
- Autoimmune disease testing – includes coeliac disease, hashimoto’s thyroiditis, autoimmune encephalitis, lupus, type 1 diabetes, etc.
Infection, autoimmune disease linked to depression
- Don’t forget to exercise and eat healthy! I really mean it, you just really need to do it, there is no other way…
Depression and anxiety: Exercise eases symptoms
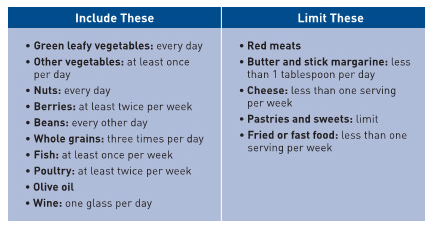
Mediterranean diet tied to lower risk of depression