I think this is a very important topic. There is now sufficient evidence to indicate that people with specific variations of genes CYP2D6, SLC6A4, and HTR2A, are unlikely to respond to SSRIs. The evidence indicates that especially Caucasian females are unlikely to respond to SSRIs, if they have the genes SLC6A4 S/S and HTR2A G/G. Evidence also shows that they may not respond to SNRIs as well.
If you are in this population, I wonder if your psychiatrist spoke to you about this. I think it’s a pretty big deal, given the sufficient evidence for Caucasians. I am an Eastern European female, and I had no response at all to any SSRIs or SNRIs, or any medication in general so far. I had trials of mirtazapine, sertraline, abilify, latuda, risperidone, olanzapine, fluoxetine, pristiq, cymbalta, and seroquel. I was then referred to a more specialized psychiatric hospital, and they performed genetic testing for me. The results indicated that I have SLC6A4 S/S and HTR2A G/G genes. The medical records state the following:
SLC6A4 S/S Homozygous for the short promoter polymorphism of the serotonin transporter gene. The short promoter allele is reported to decrease expression of the serotonin transporter compared to the homozygous long promoter allele. The patient may experience a delayed response with selective serotonin reuptake inhibitors, or may benefit from non-selective antidepressants.
HTR2A G/G Homozygous variant for the G allele for the serotonin receptor type 2a. Two copies of the G allele. This genotype has been associated with an increased risk of adverse drug reactions with certain selective serotonin reuptake inhibitors.
CYP2D6 intermediate metabolizer – Higher plasma concentrations may increase the probability of side effects. Consider a lower starting dose and slower titration schedule as compared with normal metabolizers.
I think given that I have not responded to any of the medications (each one was tried for over 8 weeks), and these test results, it’s pretty clear that I am very unlikely to respond to any other SSRIs or SNRIs. I had a very good neuropsychiatrist at the psychiatric hospital, but unfortunately I was transferred to another hospital due to pregnancy. Now I have a psychiatrist who is a resident, so she does not have a lot of experience. I was prescribed lamotrigine and fluoxetine. I think the lamotrigine makes sense, given that I have no tried it, but she only gave me 25mg per day. I don’t think the fluoxetine makes sense, because it’s an SSRI, and I have already tried it. I also stopped sleeping starting the first day I began to take it. I have been sleeping only 3-4 hours a day since I started it 8 days ago.
I wonder if anyone had a good doctor who discussed with them genetic testing and what were their suggestions? What are the options if there is no response to SSRIs and SNRIs? I don’t think my resident psychiatrist has enough experience in this.
Hello everyone, I just wanted to share my current depression regimen and some situation info, in case anyone has similar health issues. I have experienced many hospitalizations since 2015, including involuntary psychiatric hospitalizations. Finally in 2017 I was diagnosed with autoimmune encephalitis (brain inflammation), as well as autoimmune thyroiditis. I was treated with intravenous corticosteroids and that led to some improvement. I continue to experience health issues, but I have made several life style changes that have helped me and that I wanted to share. Again, I was diagnosed with autoimmune disease, and my neuropsychiatrist believes that the encephalitis greatly contributed to my depression. Clearly it’s not the case for everyone, so I am not stating that this should work for all. I have been doing better since these changes, I was able to complete a graduate degree, get back to painting, and started writing and playing guitar again. These were huge improvements for me as I was not able to enjoy any hobbies when I had severe depression and was not able to pursue graduate courses.
I cut out all refined carbs and processed foods. There is sufficient evidence indicating that these foods contribute to inflammation. I am not doing keto or low carb, I am not trying to be very strict with myself, I enjoy all sorts of complex carbs such as baked plantains, potatoes, oatmeal, fruits, berries, etc.
Switched to low glycemic foods – this related to #1, as cutting out refined simple carbs in general does leave one with complex carbs that have lower glycemic index.
Foods that cause an immune reaction – this clearly does not occur for most people, but some do react to certain foods. I noticed that I feel physically and emotionally worse after eating gluten, dairy, or soy, so I had to drop these from my diet.
I go to sleep earlier and stay away from my laptop/phone screen after 9pm. I used to stay up late, but now I go to bed around 11pm. After 9pm I usually dim the lights in the room a bit and I read on my Kindle. Kindle Paperwhite does not emit a high amount of blue light. I also installed blackout curtains so that I spend the night sleeping in the dark.
Sleep is very important – so when I really can’t fall asleep, I do use a cannabis oil (NightNight CBN + CBD oil). But changing my diet, losing weight, and going to bed earlier, did reduce my insomnia, so I don’t need the oil every day.
Significantly decreasing my caffeine intake – personally for me it did lower my anxiety and the occurrence of panic attacks, I now only have green tea in the afternoon, otherwise I drink rooibos tea, water, kefir, decaf tea.
Intermittent fasting – I do fell less brain fog and more clear headed when I am not eating the whole day. I used to surf the internet at 1am eating Sweet & Salty bars. Then my mind would go into dark places and I would start reading about serial killers. Now I eat two to three meals a day between 9am and 5pm, I fast for 16-18 hours a day.
Seeing a psychologist – going through CBT and DBT did help, and this related to #5. I still experience racing thoughts, anxiety, and other issues, but I can now more easily choose to not follow my thoughts. For example – I did used to read a lot about US serial killers and then I would freak myself out and I would start to think that someone could climb through the window. Now I choose more what I read – should I keep reading about mass murders? What is the point of that for me? Will that change anything for the better?
Sunlight – I try to get some sunlight each morning, if I have no energy to come out, I still stick out of the window and get some sunlight on my face.
Exercise – I experience certain pains due to autoimmune disease, and fatigue, so I don’t do extensive exercise, but I do yoga at home. And by exercise I don’t mean that I do a whole hour after work, I do certain yoga poses occasionally throughout the day. I think that’s still better than no exercise.
Shrooms – I did several shroom trips, at home alone, after I was treated for encephalitis. I haven’t done shrooms for a while due to pregnancy and breastfeeding, but the positive antidepressant effects of the trips still remain for me.
CBT, again – accepting that some days are better than others, some are worse, but also seeing the positive – in general I am doing much much better now than in 2016. I am female, hormones fluctuate, I do feel worse during the luteal phase, but I experience a lot more enjoyable moments than before my steroids treatment and this lifestyle change.
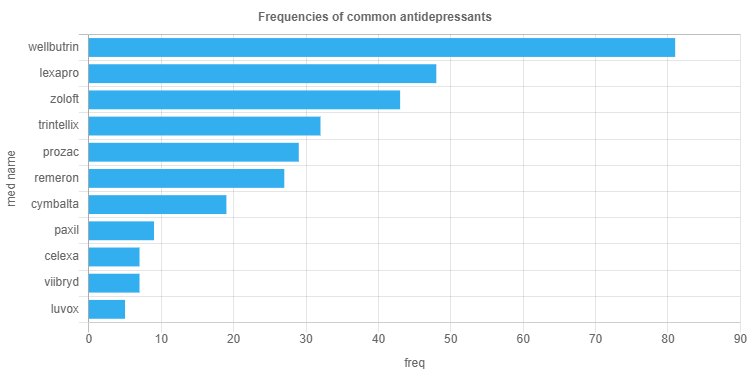
Next we will create some plots with javascript. For example, it would be interesting to see how often specific psychotropic medications and supplements are mentioned in the text data. Below is a chart with frequencies of the most common antidepressant medications. The counts were performed by combining the frequencies of the brand name and the chemical name (for example Wellbutrin count is wellbutrin (54) + bupropion (27) = 81).
The data was generated using python and exported as a .csv file, with columns ‘term’ and ‘freq’.
function makeChart(meds) {
// meds is an array of objects where each object is something like
var hist_labels = meds.map(function(d) {
return d.term;
});
var hist_counts = meds.map(function(d) {
return +d.freq;
});
arrayOfObj = hist_labels.map(function(d, i) {
return {
label: d,
data: hist_counts[i] || 0
};
});
sortedArrayOfObj = arrayOfObj.sort(function(a, b) {
return b.data - a.data;
});
newArrayLabel = [];
newArrayData = [];
sortedArrayOfObj.forEach(function(d){
newArrayLabel.push(d.label);
newArrayData.push(d.data);
});
var chart = new Chart('chart', {
type: "horizontalBar",
options: {
maintainAspectRatio: false,
legend: {
display: false
}
},
data: {
labels: newArrayLabel,
datasets: [
{
data: newArrayData,
backgroundColor: "#33AEEF"
}]
},
options: {
scales: {
yAxes: [{
scaleLabel: {
display: true,
labelString: 'med name'
}
}],
xAxes: [{
scaleLabel: {
display: true,
labelString: 'freq'
}
}],
},
legend: {
display: false
},
title: {
display: true,
text: 'Frequencies of common antidepressants'
}
}
});
}
// Request data using D3
d3
.csv("med_list_counts_df.csv")
.then(makeChart);
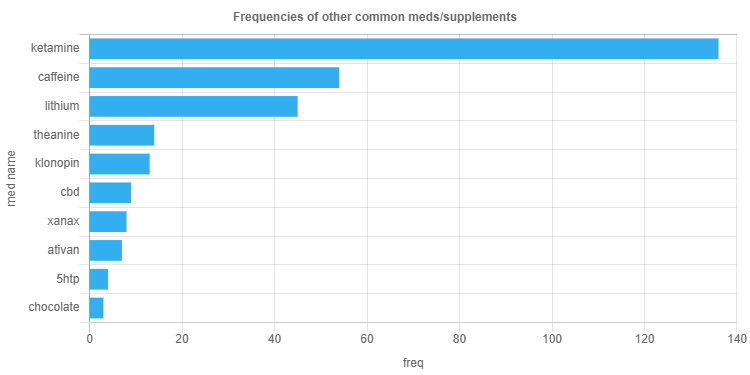
We can generate charts with other medication/supplement lists using the same code. Below is a plot with frequencies of common antipsychotics. As you can see, antipsychotics are not mentioned that frequently as antidepressants, and a lot of names in the input list were not mentioned at all (such as haldol or thorazine), and therefore they do not show up in the chart.
Other medications and common supplements mentioned:
In the previous posts we applied LDA topic modeling to text documents from data collected from the subreddit depressionregimens. Here I will continue with the results from the derived topics model – obtaining the most representative text for each topic. As was stated, the chosen model has ten topics, and LDA assumes that each document is composed of multiple topics, with each topic being assigned a probability. Each topic is composed of multiple words, with each word assigned a probability.
Since each document is composed of multiple topics, for each topic we can find a document with the highest probability for that topic, therefore that will be our most representative document.
“Blank Mind Syndrome” – Sub group of specific symptoms including: – Loss of Internal Monologue, lack of coherent automatic thoughts, no track of time passage, lack of self insight – Depersonalisation/Derealization Feeling detached, having no “sense of self”, missing mental features, having no emotional autobiography, feeling as if every day is the same, loss of relationship or emotional attachments, feeling detached from external reality – Cognitive Decline, Loss of Visual imagination, inability to think in a deep or complex way, inability to hold information, loss of past learned skills and knowledge. – Complete Lack of goal-directed motivation, having no automatic self direction, no long term goals – Anhedonia – inability to enjoy or derive pleasure, nothing to look forward to, no bodily joy, satasfaction and so on – Lack of atmosphere/deepness of the outside reality, inability to appreciate beauty, things look flat and insignificant. All symptoms in various severity of course, It’s time to talk, what is this condition exactly, Did you suffer from depression your entire life? Is this episodic? how are you planning to solve it? how did you acquire it? had any professional been aware of it? Is it medication induced? Is there any outside outlet acknowledging this specific phenomena? How much time do you suffer from it? What were you diagnosed with? Was it sudden or progressively? Had anything helped at all? Would you join a group for people suffering the same condition? Is anyone interested in doing so? Please do respond!
Topic 2
people 0.044, depression 0.037, doctor 0.028, psychiatrist 0.020, make 0.020, bad 0.016, therapy 0.016, therapist 0.015, find 0.014, problem 0.013
I talked to him today, he says all my problems are my choice and I choose to be lazy, suicidal, depressed etc. Is he right?,Dude… if he believes this then he must also believe that his career is total quackery. Get a new psychiatrist immediately. What a piece of shit.,absolutely not, please get a new psychiatrist!! you don’t choose to be suicidal or depressed, and in my experience, depression causes laziness more often than not. it’s worrisome that a professional outright said this to you and honestly I would report him if you can. that’s such a harmful thing to say to anyone suffering from such issues and to say it to the wrong person could be really catastrophic. i’m sorry he’s a dick to you, don’t listen to his bullshit. if it was so easy as to choose not to be depressed then nobody would fucking be depressed. it’s like he thinks people enjoy feeling this way ugh,OMG please please PLEASE never go back there. I once had a psychiatrist tell me I was gonna end up on a street corner with a sign (spoiler alert: I have a career and own a house). I got up and left and never looked back. Remember that YOU are a huge part of your mental health journey. It’s a collaborative effort between you, your psychiatrist, therapist (if you have one), and any other professional you choose to involve. You always have a say, and if something doesn’t seem right, you don’t have to go along with it. Your feelings are ALWAYS valid—don’t ever let anyone tell you differently. You are not alone in this. So many of us are depressed, anxious, suicidal, attention deficit, bipolar, lazy…these are NOT choices. Who would choose to be this way? There are plenty of helpful professionals out there, just make sure you screen them carefully. I believe in you and wish you well!!! …
Topic 3
day 0.037, thing 0.035, feel 0.033, make 0.024, find 0.017, good 0.016, exercise 0.016, eat 0.013, walk 0.013, lot 0.013
Wanted to share something that I’ve recently found to help when I’m struggling to find motivation to complete basic chores. This one specifically deals with laundry, but it can apply to other tasks as well. If you’re like me, you can have laundry sitting there for weeks not being put away. The mountain of clothing is so overwhelming that I just ignore it all together. I’m also an all-or-nothing person; I just wait and wait until a good day when I’ll have enough energy to get it done. Those days are exceedingly rare, so that mountain of clothes will sit there for a loooong time, stressing me out and depressing me even more. I’m trying to switch my mindset to not feeling like I need to take on such giant tasks all at once. I decided to break up the tasks into smaller ones. For the mixed load of laundry that needed to be put away, I told myself I only need to put away the socks and underwear today. Then tomorrow I put away the shirts. The next day, fold pants, and the next everything else that goes on hangers. These smaller tasks only take like 5-10 minutes each, and it’s satisfying to see the pile of clothes dwindle every day versus sit there ominously for several weeks. If you’re feeling overwhelmed, break up your tasks into very small, easily attainable goals. Go easy on yourself and do what you can for the day. Even just the tiniest amount of progress is a good thing.,great advice. Anytime you get anxiety over a task or a situation seems to complex or overwhelming. Just break in down into manageable pieces. Doing SOMETHING is always better than nothing even if it seems like too little or not enough or w/e.,I saw a meme about ‘anything worth doing is worth doing badly’ that addresses this. I try and remember that some days. Us perfectionists want to always do 100%. But in a lot of things (not everything, obviously, just as a general rule) doing 50% of the job, or 90% of the job, is way better then the 0% of the job we do because of that crippling dedication to doing 100%. Not an excuse for doing bad jobs on the stuff that really matters, but can be a much healthier way to approach doing general day-to-day stuff…
Hey y’all, this is a repost of the stickied post made by /u/jugglerofworlds, who appears to have deleted their account and their post along with it. I’ve edited it a little and will continue to keep it updated as needed. Suggestions are welcome. As the former post was, I’m trying to keep this confined to prescription medications, and not natural/herbal remedies (though I recognize that they definitely can be helpful means of treatment). I’m also typically avoiding medications that have been withdrawn from the market and thus aren’t really prescribed. In a future revision of this post I hope to add an additional column featuring which medications are available where, as some of these are approved in European countries but not in the U.S., and vice versa. # Icon key * ✔️ = approved to treat condition by a regulatory agency (FDA, EMA, ANSM, etc) * ➕ = approved as an adjunct treatment by a regulatory agency, to be used in combination with other medications to treat a condition (may or may not be used off-label as a monotherapy) * 🏷️ = Off label use; widely prescribed for condition but not necessarily rigorously studied for it * ⚠️ = experimental medication; in FDA Phase III trials or pending approval # Selective Serotonin Reuptake Inhibitors (SSRIs) |Generic name|Brand name(s)|Treats depression|Treats anxiety| |:-|:-|:-|:-| |citalopram|Celexa|✔️|🏷️| |escitalopram|Lexapro|✔️|✔️| |fluoxetine|Prozac|✔️|✔️| |fluvoxamine|Luvox/Luvox CR|✔️|✔️| |paroxetine|Paxil/Paxil CR|✔️|✔️| |sertraline|Zoloft|✔️|✔️| # Serotonin Modulator and Stimulators (SMS) |Generic name|Brand name(s)|Treats depression|Treats anxiety| |:-|:-|:-|:-| |vortioxetine|Trintellix|✔️|🏷️| |vilazodone|Viibryd|✔️|🏷️| # Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) |Generic name|Brand name(s)|Treats depression|Treats anxiety| |:-|:-|:-|:-| |venlafaxine|Effexor/Effexor XR|✔️|✔️| |desvenlafaxine|Pristiq|✔️|🏷️| |duloxetine|Cymbalta|✔️|✔️| |milnacipran|Savella|✔️|✔️| |levomilnacipran|Fetzima|✔️|🏷️| |atomoxetine|Strattera|⚠️|⚠️| # Tricyclics (TCAs) ## TCAs with a preference for serotonin |Generic name|Brand name(s)|Treats depression|Treats anxiety|…
Topic 5
treatment 0.035, ketamine 0.028, year 0.022, work 0.021, drug 0.017, hope 0.015, hear 0.012, lithium 0.011, people 0.010, infusion 0.009
https://www.washingtonpost.com/health/2019/03/06/biggest-advance-depression-years-fda-approves-novel-treatment-hardest-cases The Food and Drug Administration approved a novel antidepressant late Tuesday for people with depression that does not respond to other treatments — the first in decades to work in a completely new way in the brain. The drug, a nasal spray called esketamine, has been eagerly anticipated by psychiatrists and patient groups as a powerful new tool to fight intractable depression. The spray acts within hours, rather than weeks or months as is typical for current antidepressants, and could offer a lifeline to about 5 millionpeople in the United States with major depressive disorder who haven’t been helped by current treatments. That accounts for about one in three people with depression. “This is undeniably a major advance,” said Jeffrey Lieberman, a Columbia University psychiatrist. But he cautioned much is still unknown about the drug, particularly regarding its long-term use. “Doctors will have to be very judicious and feel their way along,” he said. The label for the drug will carry a black box warning – the most serious safety warning issued by the FDA. It will caution users they could experience sedation and problems with attention, judgment and thinking, and that there’s potential for abuse and suicidal thoughts. People who take esketamine will have to be monitored for at least two hours after receiving a dose to guard against some of these side effects…
Topic 6
work 0.053, anxiety 0.030, mg 0.025, bad 0.020, high 0.020, vitamin 0.018, diet 0.015, supplement 0.014, post 0.012, literally 0.011
About 3 or 4 years ago, I developed a severe form of anxiety disorder where it manifested in panic attacks characterized by intense bouts of nausea, gagging, and retching. It didn’t usually get bad enough to get to vomiting, though it did in a few instances (in which I went to the hospital afterwards). My body responds to stress naturally by gagging and nausea. So imagine being anxious all the time but also NAUSEOUS 24/7, and I mean literally 24/7 without any respite. At times I was seriously considering suicide because of how bad I felt all the time every day. The whole thing started I think because I had to present at a large conference with thousands of people in attendance, and I had a very bad experience being insulted by some people at a previous iteration of this conference years ago. I was commuting to work one day (before the conference) and suddenly got this massive bout of nausea where I felt like I was dying. I realized however that this was my body telling me I have stagefright. I expected my nausea to evaporate once I finished speaking, as it usually would have in the past. Except that it didn’t. It stayed, and remained with me for years. I tried everything but avoided antidepressants for the longest time due to the bad rep they get. I tried the following medications: * Ginger – in various forms – for nausea (didn’t work) * Peppermint – in various forms – for nausea (didn’t work) * Ondansetron (zofran) – 4 mg; as needed – for nausea (didn’t work) * Chlordiazepoxide/clidinium bromide (librax) – 5 mg; once daily – for nausea and anxiety (didn’t work) * Pyridoxine/doxylamine (diclectin) – 10 mg pyridoxine, 10 mg doxylamine; 2 tablets at bedtime – for nausea (didn’t work) * Metoclopramide – 1 tablet daily – for nausea (didn’t work) * Domperidone – 10 mg; once daily – for nausea (didn’t work) * Propranolol – 10 mg; twice daily – for anxiety (didn’t work) * Prochlorazapine – 10 mg; twice daily – for nausea (didn’t work) * Lorazepam (Ativan) – 1 mg; 1 tablet at bedtime – for anxiety (didn’t work; just made me really sleepy) * Pantoprazole (Tecta) – 1 tablet daily – for nausea (didn’t work) * Dimenhydrinate (Gravol) – 1 tablet as needed – for nausea (didn’t work) * Nabilone (cesamet) – 0.5 mg as needed – for nausea (worked for nausea but not anxiety, and gave me a really uncomfortable high) * Clomipramine (Anafranil) – 10 mg. once daily – for anxiety (didn’t try properly due to side-effects) I was afraid even of getting out of my own house. I was afraid of meeting people. I was afraid of leaving my own room – the only place where I felt somewhat at ease and the nausea wasn’t THAT bad. The only thing that worked somewhat to relieve the nausea was chewing on things, whether that meant food at mealtimes, or fennel seeds, or sucking on mints/cough drops. So I carried mints and fennel seeds with me at all times no matter where I was – including in the washroom in my own house and even when I wanted to take a shower I had to have them nearby otherwise I would literally throw up in the shower. But these were not long-term cures to my problem and only a short alleviation of the symptoms (and not that effective if I was more anxious than usual). I somehow graduated from university with a degree in neuroscience and fought through this nausea-anxiety for 2 years doing so. My graduation ceremony – which was supposed to be a happy occasion – was marred by constant nausea and me going through at least 3 entire tins of mints because my body handles excitedness the same way as it does for anxiety. Literally nothing was working and I was at my wit’s end. So I went downtown Toronto and bought CBD oil from a dispensary. I only did this because I was literally desperate, even though I had never done any recreational drugs in my life upto that point (except caffeine), and even though I had a horrible experience with nabilone (synthetic THC for cancer patients to reduce their nausea) so I was really kind of anxious about even using that. But it worked…
Text data (top posts and top comments for those posts) was downloaded from the subreddit depression regimens (https://www.reddit.com/r/depressionregimens/). Data was grouped by post id, in total there were 101 such ids, therefore 101 text documents. After collecting the data, the following data cleaning steps were performed:
any emails were removed from text
urls were removed (http and www)
common contractions were expanded (‘ain’t >> ‘is not’; ‘bday’ >> ‘birthday’; ‘don’t’ >> ‘do not’; etc.)
new line characters were removed
single quotes were removed
After the data cleaning steps were complete, sentences were tokenized into words, and punctuation was removed. English stop words were removed from documents. Python’s gensim.models.phrases.Phraser() was used in order to detect common phrases (bigrams). Lemmatization was then performed and part of speech tagging (POS). Only lemmatized words with certain POS tags were kept, including nouns, adjectives, verbs, adverbs, and proper nouns. Proper nouns were kept in case medication or supplement names get tagged as such. We are interested in how reddit users describe their experiences with certain psychotropic medications and supplements, and therefore the chosen POS tags are the ones that are relevant for descriptions.
An example of an original post is presented below. As a human, we can decipher that the post below is about ketamine and that the user had a positive experience with this treatment. We would be interested in the verbs, adverbs, adjectives, and nouns, that the author used to describe their experience.
I wanted to post this to give hope to those who need a little extra. I know how excruciating both having and battling treatment options for depression and anxiety can be. I’ve seen what I thought was rock bottom. I’ve been to my actual rock bottom, but I am free now.
One year ago, I was sitting in the recliner at my local ketamine clinic receiving my first infusion. The day before I had outlined my plan for suicide and had all my affairs in order, but a friend I had confided in about my depression had a “feeling” I was in a very dangerous place inside my head. I don’t know how she knew what I was planning, but thank goodness she had the foresight and the strength to push me to try one. more. thing. I had heard (and shared) quite a few podcasts from people who had been through treatment, administered the treatments, and even those who had been doing the research behind it all. had been chatting about ketamine as a potential treatment since nothing else had ever worked. She researched clinics, called them all to pick the best one, and made the appointment on an urgent basis getting me in that day.
She took me to the doctor, and after a while, I told him about my plan. I told him that I would give this a try, but this was my last try. After 25 years of my brain being a lab rat for every pill imaginable, years and years of therapy and everything else you can imagine, I was just so tired. He was sympathetic, caring and sat with me for quite a while. Then he started that first IV.
I won’t bore you with all the details of treatment (feel free to ask), but I can say that after the first treatment – one year ago today – I didn’t want to die anymore. I haven’t wanted to since. From time to time, the depression will creep in a little too much for comfort, but I have a lot of self-care tricks to help me get through it. And if It comes down to it, I go in for a booster treatment. In the past year, I have had 11 infusions. The last 3 were to help me get off the last, and most difficult antidepressant that I ever took. Now, I’m on a very low dose of Lexapro, which I honestly doubt I even need. But I’m stable. I actually know what happiness feels like. And most importantly, I’m alive. Thanks for reading.
After we perform the steps described above – data cleaning, removing stop words, lemmatization, and keeping only terms with specific POS tags, extract common bigrams, the post above results in the following:
want post give hope need little extra know excruciating battle treatment option depression anxiety see think rock bottom actual rock bottom free year ago sit recliner local ketamine clinic receive first infusion day outline plan suicide affair order friend confide depression feel dangerous place head know know plan thank goodness foresight strength push try thing hear share quite podcast people treatment administered treatment even research chat ketamine potential treatment else ever work research clinic call pick good make appointment urgent basis get day take doctor tell plan tell would give try last try year brain lab rat pill imaginable year year therapy else imagine tired sympathetic caring sit quite start first bear detail treatment feel free ask say first treatment year ago today want die anymore want time time depression creep little much comfort lot self_care trick help come go booster treatment year infusion last help last difficult antidepressant ever take low_dose lexapro honestly doubt even need stable actually know happiness feel importantly alive thank read
In regards to topic modeling, we are interested in the general topics that are discussed in this particular subreddit, Latent Dirichlet Allocation (LDA) can be used specifically for this sort of task. LDA is an unsupervised method for finding topics in text data. Our text is composed of documents, in this case each document is a combination of a post and top comments for a specific post id. LDA assumes that each document is composed of different topics and each topic is composed of different words. Therefore documents can contain overlapping topics and topics can contain overlapping words, but the probabilities for those topics and words will be different.
Since the problem is unsupervised, there are no labels, just text, and we don’t know how many topics there are in our subreddit. There is no exact formula to determine the optimal number of topics for the LDA model. One common way, that we will implement here, is to loop through different number of topics and calculate coherence scores. Then we should choose the model with the highest coherence score. In this specific case, I implemented models for 2, 4, 8, …, 14 topics, and plotted the corresponding coherence scores. As we can see from the chart, the highest value occurs when the number of topics is four, also we see peaks at 10 and 12 topics.
Now let’s see what the topics are.
Number of topics = 4
Topic 1 words
Word prob
Topic 2 words
Word prob
Topic 3 words
Word prob
Topic 4 words
Word prob
feel
0.037
day
0.042
depression
0.017
depression
0.019
thing
0.026
work
0.024
effect
0.014
people
0.017
depression
0.022
feel
0.020
antidepressant
0.013
year
0.016
make
0.021
time
0.020
ssris
0.012
give
0.016
life
0.019
sleep
0.018
doctor
0.012
treatment
0.015
time
0.013
good
0.014
anxiety
0.010
month
0.013
bad
0.013
thing
0.012
side_effect
0.010
start
0.013
good
0.012
start
0.010
mg
0.010
find
0.012
lot
0.010
bed
0.009
drug
0.009
hope
0.012
depressed
0.010
exercise
0.009
psychiatrist
0.009
ketamine
0.011
If we choose 10 topics:
Topic 1 words
Word prob
Topic 2 words
Word prob
Topic 3 words
Word prob
Topic 4 words
Word prob
Topic 5 words
Word prob
feel
0.039
people
0.044
day
0.037
ssris
0.027
treatment
0.035
year
0.026
depression
0.037
thing
0.035
antidepressant
0.024
ketamine
0.028
thing
0.022
doctor
0.028
feel
0.033
effect
0.024
year
0.022
symptom
0.020
psychiatrist
0.020
make
0.024
drug
0.022
work
0.021
brain
0.019
make
0.020
find
0.017
side_effect
0.020
drug
0.017
start
0.018
bad
0.016
good
0.016
depression
0.019
hope
0.015
time
0.017
therapy
0.016
exercise
0.016
serotonin
0.016
hear
0.012
make
0.015
therapist
0.015
eat
0.013
prescribe
0.014
lithium
0.011
issue
0.015
find
0.014
walk
0.013
treat
0.013
people
0.010
lot
0.014
problem
0.013
lot
0.013
ssri
0.012
infusion
0.009
Topic 6 words
Word prob
Topic 7 words
Word prob
Topic 8 words
Word prob
Topic 9 words
Word prob
Topic 10 words
Word prob
work
0.053
time
0.033
sleep
0.053
experience
0.039
life
0.062
anxiety
0.030
make
0.028
day
0.037
day
0.030
feel
0.030
mg
0.025
depression
0.015
time
0.030
feel
0.029
depression
0.029
bad
0.020
long
0.015
bed
0.024
depression
0.024
thing
0.020
high
0.020
call
0.014
start
0.024
mind
0.020
find
0.019
vitamin
0.018
depressed
0.014
feel
0.023
give
0.017
good
0.017
diet
0.015
feeling
0.013
morning
0.020
month
0.017
live
0.017
supplement
0.014
people
0.013
wake
0.018
good
0.015
bad
0.014
post
0.012
read
0.013
night
0.014
week
0.013
change
0.014
literally
0.011
focus
0.013
hour
0.013
back
0.012
year
0.013
I think that even with this small sample size – 101 top posts and corresponding top comments, LDA results provide us with a good understanding of what users discuss in the depressionregimens subreddit. There are discussions about life, feeling depressed, for how long the depression has been going on (mentions of week/month/year), mentions of how the day goes (Topic 7), mentions of specific treatments (Topic 4), supplements (Topic 5), SSRIs and side effects (Topic 3), exercise (Topic 2).
It’s possible to then apply the chosen model to each document in order to obtain the topics distribution by document. For example, we can choose the model with 10 topics, obtain topics distribution by document, and determine the topic with the maximum probability for each document. Then we can select sample documents that have the highest probability for a given topic. If we choose topic 2, which contains the following word distribution:
We can find documents that have the maximum probability for topic 2:
“This might be an unconventional treatment considering that many of us post about their experience with various drugs. I myself struggled with mental health in the past. I can say my mental health issues in the past were to 90% biological (hormonal problems). Once I treated the causes, over time the upwards spiral in my personal wellbeing (and life in general) started again. In early twenties, my life was starting to go down the gutter. My life started to fall apart in every domain. I was severely depressed. I found out that some of my hormones were very low. I started hormone replacement. Whereas before my life was a nightmare, it has been great ever since. I could even get off the SSRIs I was on. I wrote an article about my journey. How Hormones Destroyed and Saved My Life. My dream is to live in a world where no one is held back from living an at least decent life the way I was. Even though not my fault, it is my life. And thus my responsibility. Without accepting and acting on that I just don´t know where I would be today. For sure I wouldn´t be writing this. Hope you find value in it… “
The topics distribution for this document is as follows: [1: 0.074, 2: 0.338, 3: 0.032, 4: 0.069, 5: 0.083, 6: 0.084, 7: 0.052, 8: 0.054, 9: 0.073, 10: 0.153]
Reddit is a great source of information containing posts about depression treatments, supplements, diets, and nootropics. Since only specific psychotropic medications are prescribed for depression and anxiety and go through clinical trials with large enough sample sizes, for others we only have anecdotal stories from online users. I can’t perform a randomized controlled trial for green tea matcha’s possible antidepressant qualities without a lab and a grant, but we can use natural language processing to at least summarize some information based on user’s reviews of various supplements.
Below are top ngrams (unigrams, bigrams, and trigrams), based on the text from posts and comments from the depressionregimens subreddit. For this data sample only the top posts and top comments were selected. Posts or comments of word length less than three were removed. The data sample consisted of 1,458 documents (each document being a post of a comment). Data cleaning included removing html tags, expanding common contractions, removing newlines and tabs, removing urls, spelling correction (python’s SymSpell), lemmatization, lowercasing, and removing special characters and extra whitespaces. A list of names that included supplements, neurotransmitters, antidepressants, and other psychotropic medications, was created and excluded from spell check, in order to avoid changing these words (for example we don’t want to change ‘ssris’ to ‘saris’, which is what the SymSpell library was doing).
The ngrams were selected such that each ngram appears in less than 70% of the documents. Absolute and relative frequencies were calculated for each ngram. The top unigrams were as follows: get, depression, feel, go, try, thing, day, work, take, make, help, time, good, one, also.
Examples of posts/comments (original text, before data cleaning) with these top unigrams:
I am going to write this down somewhere.. and then take steps to figure out how to work them all away…I do all of these.. The social media/phone time one is the hardest for me. Maybe I’ll invest in one of those timer boxes I can throw it into. Then I’ll have no choice but to be productive and hopefully more creative. My depression always gets so bad around shark week. So hard to sleep and stay asleep. So for a few days out of the month I really don’t have a choice on that one. But it can easily spiral out of control if I’m not putting in constant effort. I am very tired but also wired feeling right now.
Being diagnosed with terminal cancer you will probably die. There are a lot alternatives to treat depression, regular cardio, different therapy methods, drugs and non-drugs treatments (rTMS, ECT etc.), and if you try everything and nothing work, you can survive until a new treatment arrives. Anyway, I read a lot people refusing antidepressant because “side effects”, so I think depression isn’t so bad for them, Because think about this: a guy/girl with terminal cancer will take any treatment on market if he/she can pay, ignoring side effects because she/he want live.
Thanks for sharing – having a particular difficult day today, it’s nice to hear a success story. I’ve researched this in my area, seems quite expensive, hence I’ve not been able to try it, though I’ve wanted to. Has it been that way for you? Also, I’ve been told several times that those dependent on benzodiazepine medications do not respond as well (or at all) to IV ketamine, so those must be discontinued before infusions. During the 25 years of so many medicines, did you take benzodiazepines at all? > But I’m stable. I actually know what happiness feels like. And most importantly, I’m alive. Amazing to read! Thanks again for a real success story. I wish you the very best of continued health and happiness!
The top bigrams were as follows: side effect, every day, make feel, feel well, mental health, long term, year ago, depression anxiety, treatment resistant, treat depression. Below are some post/comment examples with the top bigrams:
Ketamine crushed rumination that I had been trapped in my whole life. Repeating intrusive negative thoughts of the past. Wiping out the massive, crippling fog of depression was wonderful but that side effect of stopping those negative thoughts was life altering. Glad we found it, even if I am approaching 50 years old.
I broke the sleep/ work depression routine by walking at first. Hour long walks at a quick pace, fast enough that it was challenging. Did that for a month or so. I actually managed to lose 5 pounds that first month so there was a nice bonus. It got me thinking my diet needed improving so I cut out fast food as much as I could and starting making lean meals for myself as much as I could. After another month, that “swollen” feeling you describe started to lessen. So two months in, down 12 pounds, I joined a gym but never touched free weight. Just cardio. It was more intense than walking and took a bit to adjust to the new pace. I left a sweaty mess every day. Did that for about 6 months. I was in decent shape. Down about 30 pounds overall. My brain felt clearer and I had more energy. It’s important to isolate the depression, give it less ammunition to use against you. **One way to do that is to not let it use your body against you.**
After trying over 15 different medications and several rounds of Ketamine IV infusions for my severe treatment-resistant depression, I was about to give up. On everything. I saw a couple posts on this group about how some people have had success with Trintellix, so in a last ditch effort in desperation, I talked to my doctor and started it about a month ago. Within a week my life had changed. The existential dread had lifted. I became interested in things again. For the first time since I can remember I wasn’t exhausted in the middle of the day. I had energy. I smiled. I felt some joy. And it has continued and it’s only been getting better. I think what really happened was that it gave me the jumpstart I needed to start a small exercise regimen and care about eating right, which made me feel even better. It did make me extremely nauseous for the first week but it helped to take it with food and then the side effect went away. Thank you to those who shared their experience and I hope maybe this helps someone as well. There is hope, just keep swimming.
The top trigrams were as follows: treatment resistant depression, major depressive disorder, sexual side effect, make feel good, make feel well, mental health issue, get new psychiatrist, severe treatment resistant, stay bed day, time every day. Below are some post/comment examples with the top trigrams:
Speaking from personal experience, the only type of medication that improved my symptoms were the MAOIs. These are more old school, and more dangerous. But many have said they are a life saver for treatment resistant depression. Contrary to conventional antidepressants, they don’t just boost serotonin/dopamine/norepinephrine – they also boost a range of neurochemicals such as trace amines like b-phenylethylamine, which themselves promote the release of neurotransmitters. MAOIs are so powerful that you have to watch your diet and abstain from a whole range of other drugs.
The sexual side effects, tiredness, agitation and added anxiety all pushed me away from SSRIs. I did like being numb though. Except in the genital area… that created a huge depression in itself. Been off for months now.
Wait, you’ve told your psychiatrist about this, and they didn’t do anything? If so, you need to get a new psychiatrist. I don’t want to make a diagnosis but have you considered the possibility that you might have bipolar depression? SSRIs can cause hypomania and are considered dangerous for patients with BP. That’s why I said a new doctor is in order. Thankfully, there are antidepressants that don’t cause this reaction, as well as mood stabilizers to prevent the crash you talked about. Lastly, it sounds like you’re also dealing with a lot of stuff from your past. Are you seeing a therapist right now? They can help you work through those memories and deal with the intense emotions you get in a way that makes your life better and not worse.
We can even obtain some four grams: severe treatment resistant depression, job really well respected, amazing job really well, previous alcoholism push man, girl ever meet amazing. Post/comment examples below. I really enjoyed reading the first story as I have not heard previously about diphenidine and it was interesting to find out about this substance and the user’s experience.
I meant to post about this sooner and regret not doing so, but hopefully it’s helpful to some and doesn’t break any rules I’m not aware of. I know this subreddit has a focus on safe and researched substances and realise that this is an entirely anecdotal report concerning a not very well-researched substance, but I hope it’s not a problem and think it’s valuable information for someone suffering from severe treatment-resistant depression. Back in 2015, my husband (23 years old, weight 62 kg) had been feeling severely depressed with suicidal ideation for several weeks. It got to the point where I felt I had to either call in the mental-health people (whom I knew from previous experience to be quite inept) or take a drastic pharmacological measure. I had read about the rapid and long-lasting antidepressant responses to NMDA-receptor antagonists like ketamine before, and acquired samples of two of ones that are orally active (diphenidine, as well as methoxphenidine, also known as MXP). NMDA-receptor antagonists appear to produce their antidepressant effects by causing an increase in levels of brain-derived neurotrophic factor (BDNF) that can last for days or weeks following a single dose, whereas the most commonly used antidepressants produce a similar increase in BDNF only after weeks of continuous administration, while also causing many side effects. Neither of us had ever used any kind of dissociative before, just classical psychedelics, stimulants and marijuana (while visiting a country where that’s legal), so, given his fragile psychological state, I wanted to start with a very careful small dose. Looking at people’s comments on diphenidine and methoxphenidine online, I couldn’t find anything related to attempts at therapeutic use, nor a clear consensus on a preference for either one. I ended up looking up dosage information for diphenidine, and read that 50 mg was considered a threshold dose. I first gave him 10 mg of diphenidine in a capsule the first time to be safe; as expected, that had no noticeable effects. 2 hours later I gave him another 20 mg, which still led to no noticeable effects, except possibly a very mild numbing of the senses. Another 2 hours later I gave him another 30 mg. About 15-20 minutes after this, he reported that he was maybe starting to feel slight derealisation effects. Until this point he had been playing Skyrim to try to take his mind off his bad feelings; he really wasn’t expecting this to work at all, but he trusted my knowledge of drugs and figured it couldn’t hurt to at least try it. When the effects started to set in, I told him I’d read that some people like to lie in bed while on drugs like this, and he did so. His mood didn’t seem much changed, but after lying in bed for a bit, he started talking to me about some of the things that had been bothering him. He sounded sad while talking about these things, but I tried to steer the conversation toward solutions that we could decide on that would make life more satisfying for him. After chatting for a bit, he seemed to be getting somewhat amused by the effects of the drug; he said things he touched felt very different, and everything felt strange, but not in a bad way. As we talked some more about his issues, his mood slowly lifted (I think this was around the peak of the experience, which lasted a good portion of the day), and suddenly he got a little smile on his face and said that he was starting to feel… happy. Of course this made me really happy. He started saying how things felt “solid”, “thick”, “real” and “tangible”, in contrast not only to the way things normally felt but also to the way things had been feeling to him particularly during his weeks of feeling depressed. He related this more solid experience of physical objects to an improved outlook on life. Interestingly, despite diphenidine being a dissociative drug, it appears to have triggered a reversal of symptoms of dissociation/derealisation that accompanied his depression prior to the treatment. He said he kind of felt similar to being very drunk, I assume in relation to physical coordination. He also reported feeling significant time dilation, “in a good way”. (He contrasted this with the time dilation he feels on classical psychedelics, which he tends to find uncomfortable or scary, as though a moment will last forever.) He then seemed to get a big urge to get up and do lots of tidying and cleaning around our apartment, and he started doing so; I helped. We folded clothes, organised the living room, cleaned the kitchen, stuff like that. He said that he felt like everything was being put in its place again, both physically and mentally; that his mind was tidy again. Around this point, he seemed to have this constant feeling of awe at how content he was feeling with life. This wasn’t some kind of unnatural euphoria, just a very strong feeling of contentness, which had obviously been missing from his life for a long time. Several times, he seemed to have tears in his eyes in awe of how at peace he felt with the world. Seeing someone emerge from such a deep depression in a matter of hours was really beautiful.
Several times, he hugged me and told me how grateful he was to me for finding this drug for him. I imagine the talking was therapeutic (which could also have happened without the drug, but was, I imagine, stimulated by it), but mainly I’m certain the drug caused a biochemical change in his brain that has reversed, at least for a time, the natural process that makes him prone to feeling depressed all the time. The dissociative effects did not fully diminish until he slept; he had no trouble sleeping.
Two days later I asked him how he was feeling, and he smiled and said he was feeling just fine. More than two weeks later, his depression still had not returned. This was a massive change. It seems diphenidine can be a powerful medicine. 🙂
He later took it again, this time at 60 mg in one go (about 1 mg/kg), and he felt that this reinforced the antidepressant effects, and that repeating this every few weeks would probably keep him happy in the long term, and the interval we settled on was one dose every 12 days (taken right after waking up to avoid impacting sleep the next night). In the 5 years that followed, he continued to benefit enormously from diphenidine, and he continues to take it every 12 days. Although after a while there was some tolerance and it no longer led to complete resolution of symptoms, he continues to find it well worth it. The dosage has slowly had to be raised from 60 mg 5 years ago to around 125 mg currently (by about 16% per year) to maintain a similar level of acute effects. We’ve also discovered that adding 200-250 mg of black pepper (which contains piperine, a bioavailability enhancer) in the same capsule makes it a lot more potent.
I wonder how many people commit suicide every year who could have been saved by something like this… granted not a lot of research has been done on using NMDA-receptor antagonists for this indication and there may be unknown risks, but when someone has severe depression that cannot be managed effectively with approved medication or is even ready to commit suicide, I think there’s a very strong case to be made that something like diphenidine should be tried, at least as a last resort.
Of course it’s important to be careful not to use substances like this too frequently, since they have been known to lead to addiction with very frequent use (although, having tried it myself, I personally don’t see how the effects of this particular one could be considered enjoyable by most people). But for my husband, there has been no addiction or any other ill effect over 5 years of regular use. He is now also taking the MAOI tranylcypromine (Parnate); based on the limited research that has been done, and our experience, there is no interaction between it and diphenidine, although there probably would be with various other dissociatives.
Another example with four gram:
We’ve all been there brother. I lost the best girl I’ve ever met, an amazing job at a really well respected business and a lot of good friends through my previous alcoholism. You just have to push through it man. Even making the tiniest changes in your life will snowball into a world of difference, life always finds a way of working itself out.
I have extensive experience with psych meds, first prescription being abilify and seroquel in 2015, then mirtazapine, wellbutrin, risperidone, cymbalta, trazodone, and more. None of the meds worked for me. Last trial was of fluoxetine in November, which caused severe insomnia on only 10mg, and panic attacks. In March I also tried Zembrin which is a serotonin reuptake inhibitor (SRI). Zembrin also caused panic attacks for me and increased psychotic symptoms. I decided I don’t want to touch any additional SSRIs, SNRIs, nor SRIs.
I have also tried shrooms microdosing. I found that 1-4 gram occasional trips are better for me as microdosing makes me fatigued. While on shrooms though, a lot of thoughts came to me about reducing my caffeine intake and lithium. Lithium was mentioned to me several years ago by one consulting psychiatrist, but was never prescribed. I asked my current psych about it, but she refused to prescribe it.
While I was on Zembrin in March, by mid-month I started to get more paranoid and psychotic, as I was also in luteal phase of my cycle. A lot of women with mental illness experience PME – premenstrual exacerbation of symptoms. I unfortunately experience that as well. Mid-March I decided to stop Zembrin and any other supplements I was trying – mushroom coffee, rhodiola rosea, St. John’s Wort tea. I also stopped drinking coffee in general as I think it exacerbates my mood swings. I only continued with lithium orotate supplement that I purchased, but I stopped it as well as it seemed that it was causing more frequent urination. As I stopped these supplements and my period stabilized, my mental state somewhat stabilized to a point where I could better observe myself and think about what to do next. I decided that I still wanted to try lithium, but purchased a supplement which was in a different form – liquid which contains lithium chloride, instead of the lithium orotate tablets. I chose lithium chloride because there is more existing research on it than on lithium orotate. I also made homemade CBD oil from the Avidekel strain.
Well it has been over two months since mid-March and I’ve hard a lot more days which were just ‘alright’ instead of being a struggle with intrusive thoughts and depression. I’ve felt more calm and was able to read more throughout these two months, actually finished two books, on my third now. So in general a beneficial experience so far, will see how it goes.
Very interesting lecture found on YouTube – Dr. Roger McIntyre is a quite important guy in psychiatry here in Toronto. He is a Professor of Psychiatry and Pharmacology at the University of Toronto and Head of the Mood Disorders Psychopharmacology at UHN. He is also the director of the first Ketamine Infusion Therapy Clinic for depression in the GTA.
So in this lecture, which was posted in 2016, he talked about how just elevated C-reactive protein, a sign of general inflamamtion in the body, leads to anhedonia (inability to feel pleasure), apathy, and destuction in the brain of dopamine neurons. I wish more psychiatrists would actually listen to his lectures as well. I got a feeling, from personal experience, that some psychiatrists weren’t aware about the link between inflammaion and anhedonia, because they easily prescribed antipsychotics that cause severe weight gain. Dr. McIntyre actually speaks in the lecture against easily prescribing antipsychotics for depression, as weight gain is known to increase inflammation and therefore actually cause anhedonia/dysphoria.
So basically when an antipsychotic is described for depression – the antipsychotic reduces dopamine, since that is its function, and then further you can have death of dopamine neurons through inflammation, so that can result in complete dysphoria.
Prospective studies revealed that the average weight gain during the first year of treatment was 11.7 to 13.9 lb for clozapine, 15 to 26 lb for olanzapine, 4.4 to 5.1 lb for risperidone, 6.1 to 13.3 lb for quetiapine, and less than 2 lb for aripiprazole and ziprasidone.
This post is about comparing my experiences with fluoxetine (Prozac – an SSRI), psilocybe mushrooms, lion’s mane mushroom, and yerba mate tea. Of course this is my personal experience, not a medical study. Remember that everyone is affected differently by psychoactive compounds. In fact recently my friend told me an interesting scientific theory in regards to why humans differ a lot psychologically. Have you heard of fungi that make ants climb on top of a leaf, hook themselves, and stay there without eating, basically committing ant suicide? The spores of the fungi then burst from the ant and go on to grow into new fungi. Ophiocordyceps unilateralis is called the zombie-ant fungus.
“Researchers think the fungus, found in tropical forests, infects a foraging ant through spores that attach and penetrate the exoskeleton and slowly takes over its behavior.
As the infection advances, the enthralled ant is compelled to leave its nest for a more humid microclimate that’s favorable to the fungus’s growth. The ant is compelled to descend to a vantage point about 10 inches off the ground, sink its jaws into a leaf vein on the north side of a plant, and wait for death.
Meanwhile, the fungus feeds on its victim’s innards until it’s ready for the final stage. Several days after the ant has died, the fungus sends a fruiting body out through the base of the ant’s head, turning its shriveled corpse into a launchpad from which it can jettison its spores and infect new ants.”
So what does this have to do with humans being different? The theory says that humans evolved to react differently to same psychoactive molecules in order to not become victims to simple fungi organisms. Since the infectious fungi are not very complex organisms, they can only release so many molecules. By evolving to have complex brains and having individuals react differently to the same psychoactive molecule, humans became resistant to being overtaken by simple fungi. The theory is that there is no one molecule that a fungi could produce that would make all humans act the same, stop whatever they were doing, walk to a nice moist and wooded area, lie down, and wait for fungi spores to emerge from them.
Back to fluoxetine and shrooms
Fluoxetine
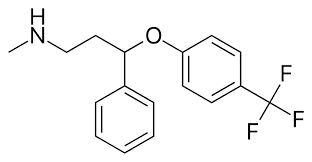
Fluoxetine is a selective serotonin reuptake inhibitor. N-methyl-3-phenyl-3-[4-(trifluoromethyl)phenoxy]propan-1-amine. It delays the reuptake of serotonin, resulting in serotonin persisting longer when it is released. Also dopamine and norepinephrine may contribute to the antidepressant action of fluoxetine in humans.
From wiki: Fluoxetine elicits antidepressant effect by inhibiting serotonin re-uptake in the synapse by binding to the re-uptake pump on the neuronal membrane to increase its availability and enhance neurotransmission. Norfluoxetine and desmethylfluoxetine are metabolites of fluoxetine and also act as serotonin re-uptake inhibitors, so increase the duration of action of the drug. Fluoxetine appeared on the Belgian market in 1986. In the U.S., the FDA gave its final approval in December 1987, and a month later Eli Lilly began marketing Prozac.
Fluoxetine is one of medications considered to be effective for PMDD (premenstrual dysphoric disorder). Also research indicates that low doses of fluoxetine could help with PMS. PMS appears to be triggered by the fall in secretion of the ovarian sex steroid hormone progesterone that occurs towards the end of the menstrual cycle and leads to a decline in its breakdown product allopregnanolone, which acts in the brain as a potent sedative and tranquilising agent. In other words, women with PMS are undergoing a type of drug withdrawal response from an in-built, tranquilising steroid chemical in their brains. New research shows that antidepressants such as fluoxetine inhibit a specific enzyme in the brain, which deactivates allopregnanolone, therefore maintaining the chemical balance of this in-built tranquiliser in the brain. Recent findings published in the British Journal of Pharmacology, show that short-term treatment with a low dose of fluoxetine immediately prior to the rat’s premenstrual period not only raised brain allopregnanolone and prevented the development of PMS-like symptoms but also blocked the increase in excitability of brain circuits involved in mediating the stress and fear responses that normally occur during this phase of the cycle.
A review of studies found that fluoxetine was more tolerabled by female patients than tricyclic amine antidepressants (Amitriptyline, Imipramine). ” In this study, a retrospective analysis of 11 randomized, double-blind, well-controlled trials was done to compare data from 427 female patients on fluoxetine and 423 female patients on TCAs. Both fluoxetine and TCAs significantly reduced the HAMD17 total mean score from baseline to end point, week 5 (fluoxetine, 24.35 to 14.37; TCAs, 24.57 to 14.43; p < 0.001). Both treatment groups were associated with significant reductions in the HAMD17 anxiety/somatization and insomnia subfactor scores. Abnormal vision, constipation, dizziness, dry mouth, and somnolence occurred more frequently (p < 0.05) in the TCA group. Insomnia and nausea were the only adverse events more common (p < 0.05) in the fluoxetine group. This study demonstrates that fluoxetine is an effective and tolerable agent for the treatment of major depressive disorder in women.”
My experience with fluoxetine – the first time that I took 10mg of fluoxetine, I felt a difference in less than three hours. It was as if I was taken out of a dark basement and into a sunny day in July. Unfortunately I also experienced insomnia that did not go away and I had a sense of apathy, in the end I stopped taking fluoxetine, but I know many women who swear by it.
Psilocybin
Next I will mention psilocybin. Psilocybin is a psychedelic compound produced by more than 200 species of mushrooms. Psilocybin is quickly converted in human body to psilocin. Psilocin is a prtial agonist for several serotonin receptors. An agonist is a chemical that binds to a receptor and activates the receptor to produce a biological response. Recently there has been increased reseach interest in psilocybin and how it could help with depression.
“A landmark study conducted by the Beckley/Imperial Research Programme has provided the first clinical evidence for the efficacy of psilocybin-assisted psychotherapy to treat depression, even in cases where all other treatments have failed. We gave oral psilocybin to 20 patients with treatment-resistant depression, all of whom had previously tried at least two other treatment methods without success. Participants had suffered from depression for an average of 18 years, with severity ranging from moderate to severe. Each patient received two doses of psilocybin (10 and 25mg) 7 days apart, accompanied by psychological support before, during, and after each session. All participants also underwent brain scans to investigate the neural underpinnings of psilocybin mechanisms of action on depression. Follow-up examinations were carried out at 5 weeks, and three and six months. Results highlights All patients showed some reductions in their depression scores at 1-week post-treatment and maximal effects were seen at 5 weeks, with results remaining positive at 3 and 6 months. Notably, reductions in depressive symptoms at 5 weeks were predicted by the quality of the acute psychedelic experience. The drug was also well tolerated by all participants, and no patients sought conventional antidepressant treatment within 5 weeks of the psilocybin intervention. While it is important to note that this was a relatively small study with no control group, placebo, or ‘blinding’ (meaning participants were fully aware what they were getting), the results are extremely encouraging and confirm that psilocybin is safe to give to depressed patients, warranting further research into this area.”
Sceletium tortuosum (Kanna) – a plant commonly found in South Africa. Laboratory studies have found that Sceletium alkaloids are selective serotonin reuptake inhibitors (SSRIs). Thus, they have the same action as pharmaceutical SSRIs such as Prozac. Animal studies have found that Sceletium can improve mood and reduce anxiety-related behaviours.
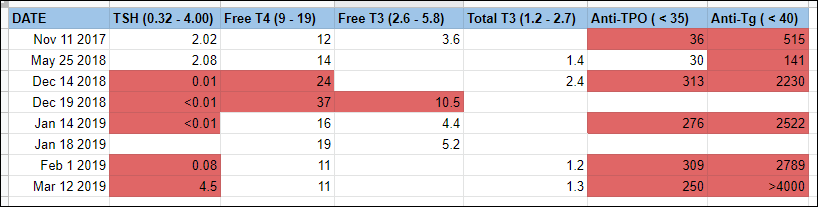
I continue to track my thyroid hormone levels and thyroid antibody levels. As my endocrinologist predicted, after a thyroid inflammation event (as indicated by ultrasound test results), and a state of hyperthyroidism, my thyroid hormone levels went the opposite way and now I am hypothyroid. I will say that for me personally the hyperthyroid state did not feel as bad as the current hypothyroid state, though I am hopeful that hypothyroidism can be treated with levothyroxine, which was recently prescribed to me. My antibody levels continue to be high and my endocrinologist stated that with Hashimoto’s autoimmune disease in general antibody levels stay chronically elevated. I might be receiving IVIG treatment soon, in April, and hopefully that will reduce the inflammation of the thyroid.
In terms of emotions, during hyperthyroidism, I did feel jittery and very hungry, but I also experienced a roller coaster of more positive emotions such as more interest in men, infatuation, desire for adventure. I can’t say that my depression went away, but I do remember having moments of making plans to travel to Guatemala to attend a Spanish course, thinking of having an affair, wanting to perform in a band with my violin. Recently with hypothyroidism, as I described in a previous post, what I had been feeling is complete disinterest and grief. As if your life is somehow passing by, the world keeps going without you. There is a feeling of slowness in your movements and speech, a sense of painful emotional weight, inability to fully engage in an activity. Well if you have experienced hypothyroidism, you might know what I’m talking about. It’s feeling lonely and yet having no energy to call someone to make plans. Thinking that in theory I do enjoy playing violin, but today doing that would be just too difficult. Exercising definitely was becoming impossible, my legs have been feeling very heavy, and my whole body in general.
Today I started levothyroxine 0.025mg and I am hopeful that this will lower my TSH and therefore relieve all the symptoms that I am experiencing, at least I am very hopeful that levothyroxine in combination with IVIG will really help. I found an interesting study in which the authors seek a TSH threshold for depression. Two thirds of the study participants were female, as expected. There were 174 hypothyroid patients who were receiving levothyroxine treatment and were considered euthyroid. “Individuals who had developed euthyroid state under treatment with levothyroxine with TSH levels of 0.5–5 MIU/L with no need for dosage change were included in the study. After comprehensive history taking, laboratory tests including TSH, T4 and T3 were performed. Beck depression questionnaire was completed for all patients by trained interviewers. TSH cut-off values based on depression was determined by Roc Curve analysis.” Basically, as I understand, the researchers wanted to find out whether there is correlation between TSH levels and depression for patients who were diagnosed with hypothyroidism and are receiving levothyroxine.
Results were the following: “According to Roc curve analysis, the optimal cut- off value of TSH was 2.5 MIU/L with 89.66% sensitivity. The optimal TSH cut- off based on severe depression was 4 MIU/L. The present study suggests that a clinically helpful TSH cut-off value for hypothyroidism should be based on associated symptoms, not just in population studies. Based on the assessment of depression, our study concludes that a TSH cutofff value of 2.5 MIU/L is optimal.” I think what they are trying to say here is that based on large population studies there was a range for normal TSH levels determined, for example on my lab tests that range is stated as 0.32 – 4.00. Their study shows though that even though my individual TSH could be within this range, it doesn’t mean that I won’t be having any hypothyroidism symptoms, such as depression. Maybe for me personally TSH of 3.80 would be too high and my mood would be influenced and I would be better off at a level of levothyroxine that would bring my TSH below 2.5. Therefore it’s important to consider the symptoms of a specific patient and not just the determined ‘normal’ range.
Also different countries and labs don’t state the same ‘normal’ ranges. In the study the TSH range is indicated as 0.5 – 5 MIU/L, while my lab states 0.32 – 4. So if I went to a doctor in another country, he could have said that my thyroid hormone levels are normal, but based on my lab’s range, my endocrinologist said that I might be becoming hypothyroid, since TSH is out of range, and therefore prescribed me levothyroxine. Also he did take into account the symptoms that I was experiencing, which is what the authors suggest – don’t just look at the TSH, how does the patient feel?