Text data (top posts and top comments for those posts) was downloaded from the subreddit depression regimens (https://www.reddit.com/r/depressionregimens/). Data was grouped by post id, in total there were 101 such ids, therefore 101 text documents. After collecting the data, the following data cleaning steps were performed:
- any emails were removed from text
- urls were removed (http and www)
- common contractions were expanded (‘ain’t >> ‘is not’; ‘bday’ >> ‘birthday’; ‘don’t’ >> ‘do not’; etc.)
- new line characters were removed
- single quotes were removed
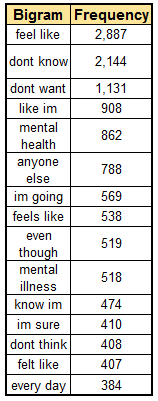
After the data cleaning steps were complete, sentences were tokenized into words, and punctuation was removed. English stop words were removed from documents. Python’s gensim.models.phrases.Phraser() was used in order to detect common phrases (bigrams). Lemmatization was then performed and part of speech tagging (POS). Only lemmatized words with certain POS tags were kept, including nouns, adjectives, verbs, adverbs, and proper nouns. Proper nouns were kept in case medication or supplement names get tagged as such. We are interested in how reddit users describe their experiences with certain psychotropic medications and supplements, and therefore the chosen POS tags are the ones that are relevant for descriptions.
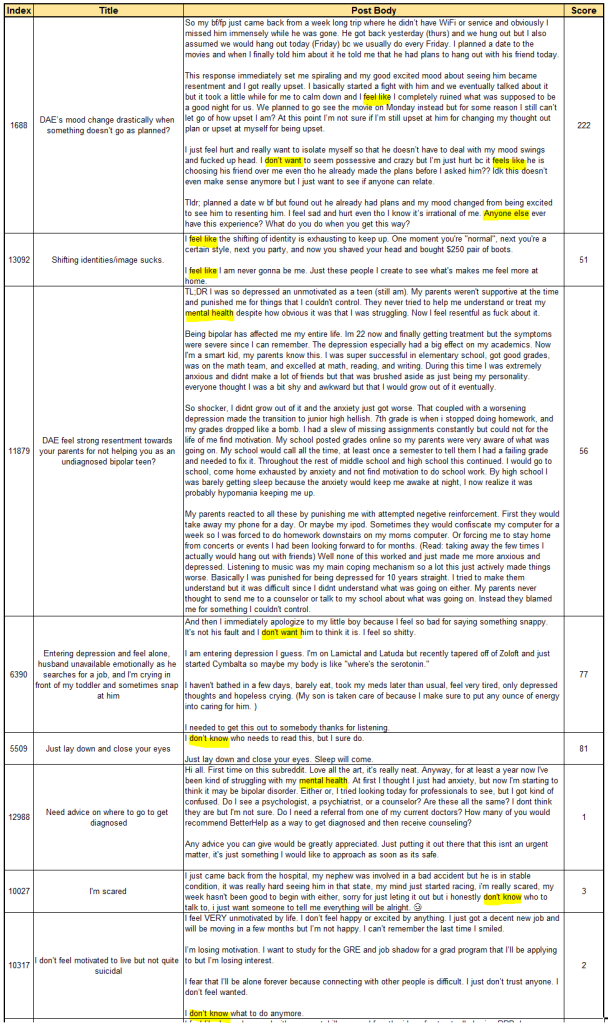
An example of an original post is presented below. As a human, we can decipher that the post below is about ketamine and that the user had a positive experience with this treatment. We would be interested in the verbs, adverbs, adjectives, and nouns, that the author used to describe their experience.
I wanted to post this to give hope to those who need a little extra. I know how excruciating both having and battling treatment options for depression and anxiety can be. I’ve seen what I thought was rock bottom. I’ve been to my actual rock bottom, but I am free now.
One year ago, I was sitting in the recliner at my local ketamine clinic receiving my first infusion. The day before I had outlined my plan for suicide and had all my affairs in order, but a friend I had confided in about my depression had a “feeling” I was in a very dangerous place inside my head. I don’t know how she knew what I was planning, but thank goodness she had the foresight and the strength to push me to try one. more. thing. I had heard (and shared) quite a few podcasts from people who had been through treatment, administered the treatments, and even those who had been doing the research behind it all. had been chatting about ketamine as a potential treatment since nothing else had ever worked. She researched clinics, called them all to pick the best one, and made the appointment on an urgent basis getting me in that day.
She took me to the doctor, and after a while, I told him about my plan. I told him that I would give this a try, but this was my last try. After 25 years of my brain being a lab rat for every pill imaginable, years and years of therapy and everything else you can imagine, I was just so tired. He was sympathetic, caring and sat with me for quite a while. Then he started that first IV.
I won’t bore you with all the details of treatment (feel free to ask), but I can say that after the first treatment – one year ago today – I didn’t want to die anymore. I haven’t wanted to since. From time to time, the depression will creep in a little too much for comfort, but I have a lot of self-care tricks to help me get through it. And if It comes down to it, I go in for a booster treatment.
In the past year, I have had 11 infusions. The last 3 were to help me get off the last, and most difficult antidepressant that I ever took. Now, I’m on a very low dose of Lexapro, which I honestly doubt I even need. But I’m stable. I actually know what happiness feels like. And most importantly, I’m alive.
Thanks for reading.
After we perform the steps described above – data cleaning, removing stop words, lemmatization, and keeping only terms with specific POS tags, extract common bigrams, the post above results in the following:
want post give hope need little extra know excruciating battle treatment option depression anxiety see think rock bottom actual rock bottom free year ago sit recliner local ketamine clinic receive first infusion day outline plan suicide affair order friend confide depression feel dangerous place head know know plan thank goodness foresight strength push try thing hear share quite podcast people treatment administered treatment even research chat ketamine potential treatment else ever work research clinic call pick good make appointment urgent basis get day take doctor tell plan tell would give try last try year brain lab rat pill imaginable year year therapy else imagine tired sympathetic caring sit quite start first bear detail treatment feel free ask say first treatment year ago today want die anymore want time time depression creep little much comfort lot self_care trick help come go booster treatment year infusion last help last difficult antidepressant ever take low_dose lexapro honestly doubt even need stable actually know happiness feel importantly alive thank read
In regards to topic modeling, we are interested in the general topics that are discussed in this particular subreddit, Latent Dirichlet Allocation (LDA) can be used specifically for this sort of task. LDA is an unsupervised method for finding topics in text data. Our text is composed of documents, in this case each document is a combination of a post and top comments for a specific post id. LDA assumes that each document is composed of different topics and each topic is composed of different words. Therefore documents can contain overlapping topics and topics can contain overlapping words, but the probabilities for those topics and words will be different.
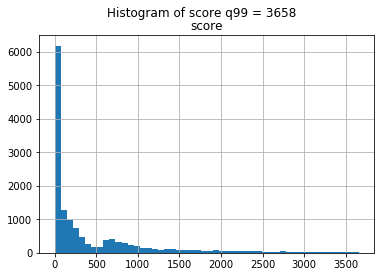
Since the problem is unsupervised, there are no labels, just text, and we don’t know how many topics there are in our subreddit. There is no exact formula to determine the optimal number of topics for the LDA model. One common way, that we will implement here, is to loop through different number of topics and calculate coherence scores. Then we should choose the model with the highest coherence score. In this specific case, I implemented models for 2, 4, 8, …, 14 topics, and plotted the corresponding coherence scores. As we can see from the chart, the highest value occurs when the number of topics is four, also we see peaks at 10 and 12 topics.

Now let’s see what the topics are.
Number of topics = 4
| Topic 1 words | Word prob | Topic 2 words | Word prob | Topic 3 words | Word prob | Topic 4 words | Word prob |
| feel | 0.037 | day | 0.042 | depression | 0.017 | depression | 0.019 |
| thing | 0.026 | work | 0.024 | effect | 0.014 | people | 0.017 |
| depression | 0.022 | feel | 0.020 | antidepressant | 0.013 | year | 0.016 |
| make | 0.021 | time | 0.020 | ssris | 0.012 | give | 0.016 |
| life | 0.019 | sleep | 0.018 | doctor | 0.012 | treatment | 0.015 |
| time | 0.013 | good | 0.014 | anxiety | 0.010 | month | 0.013 |
| bad | 0.013 | thing | 0.012 | side_effect | 0.010 | start | 0.013 |
| good | 0.012 | start | 0.010 | mg | 0.010 | find | 0.012 |
| lot | 0.010 | bed | 0.009 | drug | 0.009 | hope | 0.012 |
| depressed | 0.010 | exercise | 0.009 | psychiatrist | 0.009 | ketamine | 0.011 |
If we choose 10 topics:
| Topic 1 words | Word prob | Topic 2 words | Word prob | Topic 3 words | Word prob | Topic 4 words | Word prob | Topic 5 words | Word prob |
| feel | 0.039 | people | 0.044 | day | 0.037 | ssris | 0.027 | treatment | 0.035 |
| year | 0.026 | depression | 0.037 | thing | 0.035 | antidepressant | 0.024 | ketamine | 0.028 |
| thing | 0.022 | doctor | 0.028 | feel | 0.033 | effect | 0.024 | year | 0.022 |
| symptom | 0.020 | psychiatrist | 0.020 | make | 0.024 | drug | 0.022 | work | 0.021 |
| brain | 0.019 | make | 0.020 | find | 0.017 | side_effect | 0.020 | drug | 0.017 |
| start | 0.018 | bad | 0.016 | good | 0.016 | depression | 0.019 | hope | 0.015 |
| time | 0.017 | therapy | 0.016 | exercise | 0.016 | serotonin | 0.016 | hear | 0.012 |
| make | 0.015 | therapist | 0.015 | eat | 0.013 | prescribe | 0.014 | lithium | 0.011 |
| issue | 0.015 | find | 0.014 | walk | 0.013 | treat | 0.013 | people | 0.010 |
| lot | 0.014 | problem | 0.013 | lot | 0.013 | ssri | 0.012 | infusion | 0.009 |
| Topic 6 words | Word prob | Topic 7 words | Word prob | Topic 8 words | Word prob | Topic 9 words | Word prob | Topic 10 words | Word prob |
| work | 0.053 | time | 0.033 | sleep | 0.053 | experience | 0.039 | life | 0.062 |
| anxiety | 0.030 | make | 0.028 | day | 0.037 | day | 0.030 | feel | 0.030 |
| mg | 0.025 | depression | 0.015 | time | 0.030 | feel | 0.029 | depression | 0.029 |
| bad | 0.020 | long | 0.015 | bed | 0.024 | depression | 0.024 | thing | 0.020 |
| high | 0.020 | call | 0.014 | start | 0.024 | mind | 0.020 | find | 0.019 |
| vitamin | 0.018 | depressed | 0.014 | feel | 0.023 | give | 0.017 | good | 0.017 |
| diet | 0.015 | feeling | 0.013 | morning | 0.020 | month | 0.017 | live | 0.017 |
| supplement | 0.014 | people | 0.013 | wake | 0.018 | good | 0.015 | bad | 0.014 |
| post | 0.012 | read | 0.013 | night | 0.014 | week | 0.013 | change | 0.014 |
| literally | 0.011 | focus | 0.013 | hour | 0.013 | back | 0.012 | year | 0.013 |
I think that even with this small sample size – 101 top posts and corresponding top comments, LDA results provide us with a good understanding of what users discuss in the depressionregimens subreddit. There are discussions about life, feeling depressed, for how long the depression has been going on (mentions of week/month/year), mentions of how the day goes (Topic 7), mentions of specific treatments (Topic 4), supplements (Topic 5), SSRIs and side effects (Topic 3), exercise (Topic 2).
It’s possible to then apply the chosen model to each document in order to obtain the topics distribution by document. For example, we can choose the model with 10 topics, obtain topics distribution by document, and determine the topic with the maximum probability for each document. Then we can select sample documents that have the highest probability for a given topic. If we choose topic 2, which contains the following word distribution:
(‘people’, 0.04), (‘depression’, 0.038), (‘doctor’, 0.028), (‘psychiatrist’, 0.020),
(‘make’, 0.020), (‘bad’, 0.016), (‘therapy’, 0.016), (‘therapist’, 0.015), (‘find’, 0.014),
(‘problem’, 0.013)
We can find documents that have the maximum probability for topic 2:
“This might be an unconventional treatment considering that many of us post about their experience with various drugs.
I myself struggled with mental health in the past. I can say my mental health issues in the past were to 90% biological (hormonal problems). Once I treated the causes, over time the upwards spiral in my personal wellbeing (and life in general) started again.
In early twenties, my life was starting to go down the gutter. My life started to fall apart in every domain. I was severely depressed. I found out that some of my hormones were very low. I started hormone replacement. Whereas before my life was a nightmare, it has been great ever since. I could even get off the SSRIs I was on.
I wrote an article about my journey. How Hormones Destroyed and Saved My Life.
My dream is to live in a world where no one is held back from living an at least decent life the way I was. Even though not my fault, it is my life. And thus my responsibility. Without accepting and acting on that I just don´t know where I would be today. For sure I wouldn´t be writing this. Hope you find value in it… “
(Can read full text at https://www.reddit.com/r/depressionregimens/comments/lef32x )
The topics distribution for this document is as follows:
[1: 0.074, 2: 0.338, 3: 0.032, 4: 0.069, 5: 0.083, 6: 0.084, 7: 0.052, 8: 0.054, 9: 0.073, 10: 0.153]
Lemmatized text:
[‘may’, ‘unconventional’, ‘treatment’, ‘consider’, ‘many’, ‘us’, ‘post’, ‘experience’, ‘various’, ‘drug’, ‘struggle’, [‘may’, ‘unconventional’, ‘treatment’, ‘consider’, ‘many’, ‘us’, ‘post’, ‘experience’, ‘various’, ‘drug’, ‘struggle’, ‘mental_health’, ‘say’, ‘mental_health’, ‘issue’, ‘biological’, ‘hormonal’, ‘problem‘, ‘treat’, ’cause’, ‘time’, ‘upwards’, ‘spiral’, ‘personal’, ‘wellbeing’, ‘life’, ‘general’, ‘start’, ‘early’, ‘twenty’, ‘life’, ‘start’, ‘go’, ‘gutter’, ‘life’, ‘start’, ‘fall’, ‘apart’, ‘domain’, ‘severely_depresse’, ‘find‘, ‘hormone’, ‘low’, ‘start’, ‘hormone’, ‘replacement’, ‘life’, ‘nightmare’, ‘great’, ‘ever’, ‘since’, ‘could’, ‘even’, ‘ssris’, ‘write’, ‘article’, ‘journey’, ‘hormone’, ‘destroy’, ‘save’, ‘life’, ‘dream’, ‘live’, ‘world’, ‘hold’, ‘back’, ‘live’, ‘least’, ‘decent’, ‘life’, ‘way’, ‘even’, ‘fault’, ‘life’, ‘thus’, ‘responsibility’, ‘accept’, ‘act’, ‘know’, ‘would’, ‘today’, ‘sure’, ‘write’, ‘hope’, ‘find‘, ‘value’, ‘opinion’, ‘replace’, ‘hormone’, ‘deficient’, ‘far’, ‘natural’, ‘also’, ‘effective’, ‘artificial’, ‘med’, ‘however’, ‘believe’, ‘hormone’, ‘deficiency’, ‘may’, ‘much’, ‘common’, ‘assume’, ‘people‘, ‘never’, ‘get’, ‘hormone’, ‘check’, ‘often’, ‘even’, ‘life’, ‘want’, ‘give’, ‘head’, ‘other’, ‘pull’, ‘trigger’, ‘medication’, ‘claim’, ‘medication’, ‘work’, ‘hormone’, ‘check’, ‘opportunity’, ‘cost’, ‘high’, ‘similar’, ‘experience’, ‘hormone’, ‘hormone’, ‘dangerous’, ‘play’, ‘make‘, ‘sure’, ‘talk’, ‘doctor‘, ‘monitor’, ‘doctor‘, ‘lock’, ‘post’, ‘people‘, ‘would’, ‘see’, ‘unlocked’, ‘pm’, ‘otherwise’, ‘leave’, ‘lock’, ‘play’, ‘hormone’, ‘medical’, ‘supervision’, ‘highly’, ‘detrimental’, ‘health’, ‘thyroid’, ‘hormone’, ‘deficient’, ‘know’, ‘other’, ‘start’, ‘take’, ‘mcg’, ‘thyroxine’, ‘treat’, ‘hypothyroidism’, ‘run’, ‘family’, ‘fog’, ‘seem’, ‘lift’, ‘agree’, ‘hormone’, ‘underrated’, ‘come’, ‘depression‘, ‘thank’, ‘share’, ‘hormone’, ‘specifically’, ‘testosterone’, ‘direct’, ‘correlation’, ‘dopamine’, ‘high’, ‘test’, ‘high’, ‘dopamine’, ‘vice’, ‘versa’, ‘generally’, ‘testerone’, ‘wellbutrin’, ‘increase’, ‘libido’, ‘endocrine’, ‘system’, ‘research’, ‘seem’, ‘lag’, ‘research’, ‘treatment’, ‘know’, ‘million’, ‘could’, ‘suffer’, ‘needlessly’, ‘ignore’, ‘op’, ‘entire’, ‘post’, ‘structure’, ‘sway’, ‘people‘, ‘way’, ‘link’, ‘closing’, ‘paragraph’, ‘also’, ‘spamme’, ‘numerous’, ‘time’, ‘different’, ‘thing’, ’cause’, ‘depression‘, ‘know’, ‘enough’, ‘dark’, ‘age’, ‘exclusive’, ‘seratonin’, ‘hormone’, ‘receptor’, ‘regulation’, ‘drug’, ‘abuse’, ‘dopamine’, ‘ach’, ‘brain’, ‘damage’, ‘gaba’, ‘glutamate’, ‘imbalance’, ‘relate’, ‘several’, ‘brain’, ‘region’, ‘receptor’, ‘site’, ‘together’, ‘hormone’, ‘conversion’, ‘chain’, ‘adhd’, ‘bp’, ‘level’, ‘bdnf’, ‘several’, ‘type’, ‘disease’, ‘additionally’, ‘low’, ‘end’, ‘hormone’, ‘scale’, ‘total’, ‘free’, ‘may’, ‘feel’, ‘symptom’, ‘other’, ‘would’, ‘conversely’, ‘man’, ‘may’, ‘almost’, ‘nil’, ‘estrogen’, ‘high’, ‘estrogen’, ‘side_effect’, ‘decent’, ‘doctor‘, ‘full’, ‘blood’, ‘panel’, ‘hormone’, ‘panel’, ‘include’, ‘ask’, ‘depend’, ‘free’, ‘go’, ‘private’, ‘cost’, ‘uk’, ‘take’, ‘important’, ‘relative’, ‘commit’, ‘find‘, ‘thyroid’, ‘level’, ‘way’, ‘back’, ‘thyroid’, ‘problem‘, ‘handle’, ‘psych’, ‘med’, ‘need’, ‘depression‘, ‘probably’, ‘lifelong’, ‘become’, ‘unmanageable’, ‘thyroid’, ‘cancer’, ‘luckily’, ‘old’, ‘easy’, ‘catch’, ‘get’, ‘point’, ‘hormone’, ‘low’, ‘find‘, ‘hormone’, ‘check’, ‘yearly’, ‘perfectly’, ‘normal’, ‘even’, ‘high’, ‘yet’, ‘still’, ‘depressed’, ‘hormone’, ‘may’, ‘help’, ‘people‘, ‘many’, ‘still’, ‘depress’, ‘physiological’, ‘duck’, ‘row’, ‘infuriate’, ‘many’, ‘doctor‘, ‘refuse’, ‘prescribe’, ‘hrt’, ‘guess’, ‘taboo’, ‘medical’, ‘school’, ‘pull’, ‘tooth’, ‘find‘, ‘decent’, ‘doctor‘, ‘even’, ‘consider’, ‘apparently’, ‘fear’, ‘cancer’, ‘induce’, ‘hormone’, ‘frankly’, ‘rather’, ‘live’, ‘good’, ‘life’, ‘even’, ‘mean’, ‘get’, ‘cancer’, ‘live’, ‘cancer’, ‘free’, ‘life’, ‘mentally’, ‘miserable’, ‘post’, ‘multiple’, ‘account’, ‘whole’, ‘time’, ‘person’, ‘post’, ‘often’, ‘article’, ‘different’, ‘account’, ‘sometimes’, ‘claim’, ‘last’, ‘year’, ‘biology’, ‘student’, ‘other’, ‘last’, ‘year’, ‘medicine’, ‘student’, ‘post’, ‘lame’, ‘excuse’, ‘lure’, ‘costumer’, ‘hormetheu’, ‘thank’, ‘share’, ‘disregard’, ‘irrational’, ‘post’, ‘intelligent’, ‘enough’, ‘determine’, ‘right’, ‘see’, ‘sort’, ‘ground’, ‘swell’, ‘business’, ‘activity’, ‘even’, ‘touch’, ‘consultation’, ‘hormone’, ‘way’, ‘business’, ‘s’, ‘even’, ‘well’, ‘talk’, ‘get’, ‘free’, ‘professsional’, ‘guidance’, ‘think’, ‘people‘, ‘stick’, ‘depression‘, ’cause’, ‘people‘, ‘pursue’, ‘treatment’, ‘may’, ‘save’, ‘life’, ‘know’, ‘firsthand’, ‘appropriate’, ‘way’, ‘respond’, ‘tell’, ‘support’, ‘other’, ‘say’, ‘mother’, ‘first’, ‘tell’, ‘hit’, ‘would’, ‘sit’, ‘kitchen’, ‘table’, ‘cry’, ‘uncontrollably’, ‘start’, ‘hrt’, ‘right’, ‘take’, ‘nurse’, ‘year’, ‘tortuous’, ‘severe’, ‘depression‘, ‘ask’, ‘do’, ‘hormone’, ‘panel’, ‘flabbergast’, ‘go’, ‘lowt’, ‘men’, ‘health’, ‘center’, ‘addition’, ‘find‘, ‘severely’, ‘low’, ‘receive’, ‘great’, ‘man’, ‘health’, ‘care’, ‘know’, ‘funny’, ‘deduce’, ‘man’, ‘mid’, ‘life’, ‘crisis’, ‘hormone’, ‘imbalance’, ‘likely’, ‘low’, ‘get’, ‘ball’, ‘bust’, ‘buy’, ‘corvette’, ‘woman’, ‘get’, ‘sympathy’, ‘go’, ‘change’, ‘enough’, ‘question’, ‘come’, ‘first’, ‘opinion’, ‘testosterone’, ‘brain’, ‘get’, ‘testosterone’, ‘shot’, ‘help’, ‘put’, ‘dent’, ‘depression‘, ‘make‘, ‘feel’, ‘well’, ‘still’, ‘leave’, ‘pretty’, ‘severe’, ‘depression‘, ‘admittedly’, ‘hormone’, ‘vitamin’, ‘could’, ‘do’, ‘aggressively’, ‘recently’, ‘do’, ‘put’, ‘brain’, ‘glide’, ‘path’, ‘depression‘, ‘amazing’, ‘think’, ‘fix’, ‘fix’, ‘brain’, ‘still’, ‘aggressively’, ‘pursue’, ‘low’, ‘hear’, ‘cortisol’, ‘kill’, ‘testosterone’]